

Impact of centralising acute stroke services in English metropolitan areas on mortality and length of hospital stay: difference-in-differences analysis
- PMID: 25098169
- PMCID: PMC4122734
- DOI: 10.1136/bmj.g4757
Impact of centralising acute stroke services in English metropolitan areas on mortality and length of hospital stay: difference-in-differences analysis
Abstract
Objective: To investigate whether centralisation of acute stroke services in two metropolitan areas of England was associated with changes in mortality and length of hospital stay.
Design: Analysis of difference-in-differences between regions with patient level data from the hospital episode statistics database linked to mortality data supplied by the Office for National Statistics.
Setting: Acute stroke services in Greater Manchester and London, England.
Participants: 258,915 patients with stroke living in urban areas and admitted to hospital in January 2008 to March 2012.
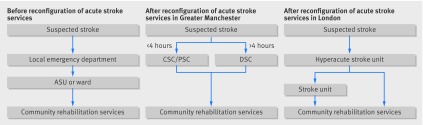
Interventions: "Hub and spoke" model for acute stroke care. In London hyperacute care was provided to all patients with stroke. In Greater Manchester hyperacute care was provided to patients presenting within four hours of developing symptoms of stroke.
Main outcome measures: Mortality from any cause and at any place at 3, 30, and 90 days after hospital admission; length of hospital stay.
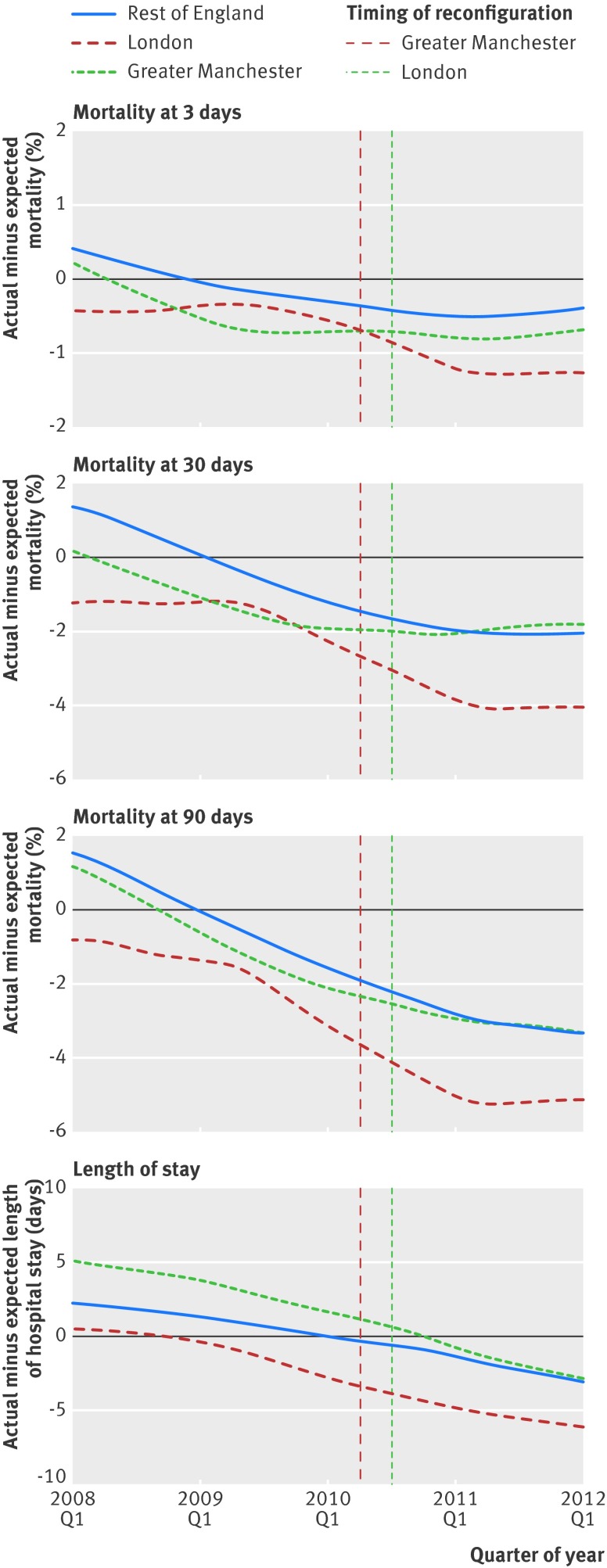
Results: In London there was a significant decline in risk adjusted mortality at 3, 30, and 90 days after admission. At 90 days the absolute reduction was -1.1% (95% confidence interval -2.1 to -0.1; relative reduction 5%), indicating 168 fewer deaths (95% confidence interval 19 to 316) during the 21 month period after reconfiguration in London. In both areas there was a significant decline in risk adjusted length of hospital stay: -2.0 days in Greater Manchester (95% confidence interval -2.8 to -1.2; 9%) and -1.4 days in London (-2.3 to -0.5; 7%). Reductions in mortality and length of hospital stay were largely seen among patients with ischaemic stroke.
Conclusions: A centralised model of acute stroke care, in which hyperacute care is provided to all patients with stroke across an entire metropolitan area, can reduce mortality and length of hospital stay.
© Morris et al 2014.
Conflict of interest statement
Competing interests: All authors have completed the ICMJE uniform disclosure form at
Figures
Comment in
-
Centralising acute stroke services: study confounded by financial investment.BMJ. 2014 Sep 23;349:g5710. doi: 10.1136/bmj.g5710. BMJ. 2014. PMID: 25249194 No abstract available.
-
Study on centralising acute stroke services provides no firm conclusions.BMJ. 2014 Sep 23;349:g5715. doi: 10.1136/bmj.g5715. BMJ. 2014. PMID: 25249287 No abstract available.
-
Authors' reply to Hill and Rudd.BMJ. 2014 Sep 23;349:g5717. doi: 10.1136/bmj.g5717. BMJ. 2014. PMID: 25249508 No abstract available.
References
-
- Mackay J, Mensah GA. The atlas of heart disease and stroke. World Health Organization, 2004.
-
- Townsend N, Wickramasinghe K, Bhatnagar P, Smolina K, Nichols M, Leal J, et al. Coronary heart disease statistics. British Heart Foundation, 2012.
-
- Langhorne P, Fearon P, Ronning OM, Kaste M, Palomaki H, Vemmos K, et al. Stroke unit care benefits patients with intracerebral hemorrhage systematic review and meta-analysis. Stroke 2013;44:3044-9. - PubMed
-
- Department of Health. National Stroke Strategy. DoH, 2007. http://clahrc-gm.nihr.ac.uk/cms/wp-content/uploads/DoH-National-Stroke-S....
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical