

Integrating mobile phones into medical abortion provision: intervention development, use, and lessons learned from a randomized controlled trial
- PMID: 25098569
- PMCID: PMC4114479
- DOI: 10.2196/mhealth.3165
Integrating mobile phones into medical abortion provision: intervention development, use, and lessons learned from a randomized controlled trial
Abstract
Background: Medical abortion is legal in South Africa but access and acceptability are hampered by the current protocol requiring a follow-up visit to assess abortion completion.
Objective: To assess the feasibility and efficacy of information and follow-up provided via mobile phone after medical abortion in a randomized controlled trial (RCT).
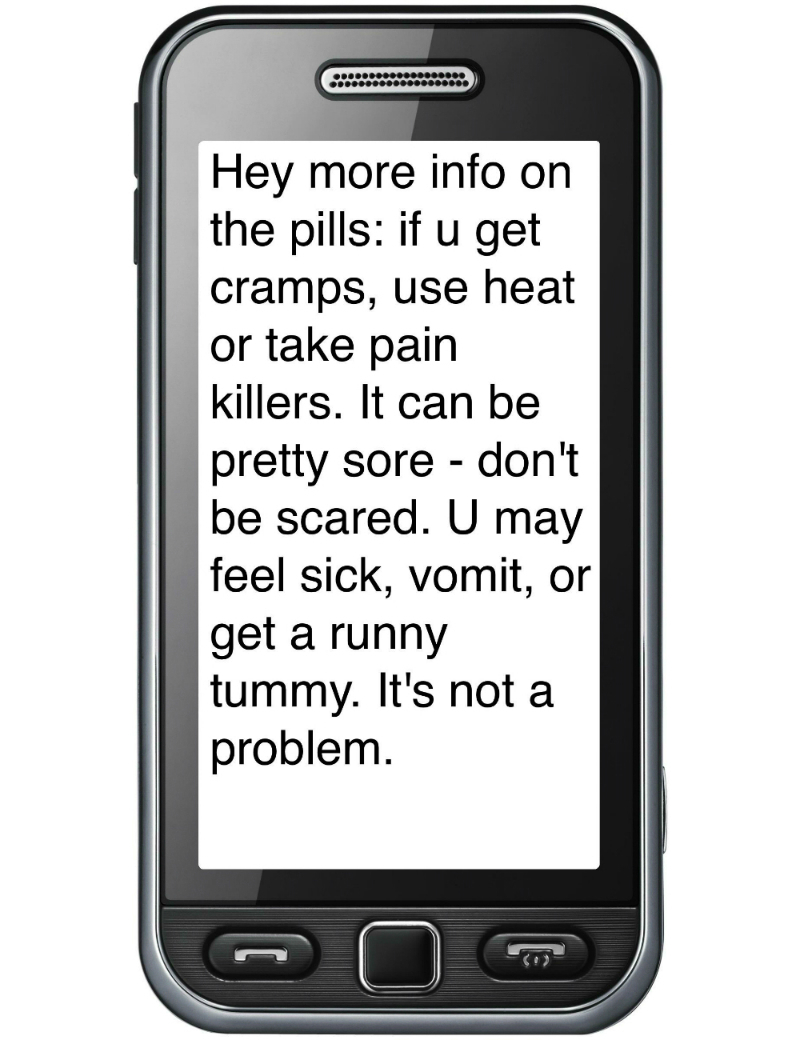
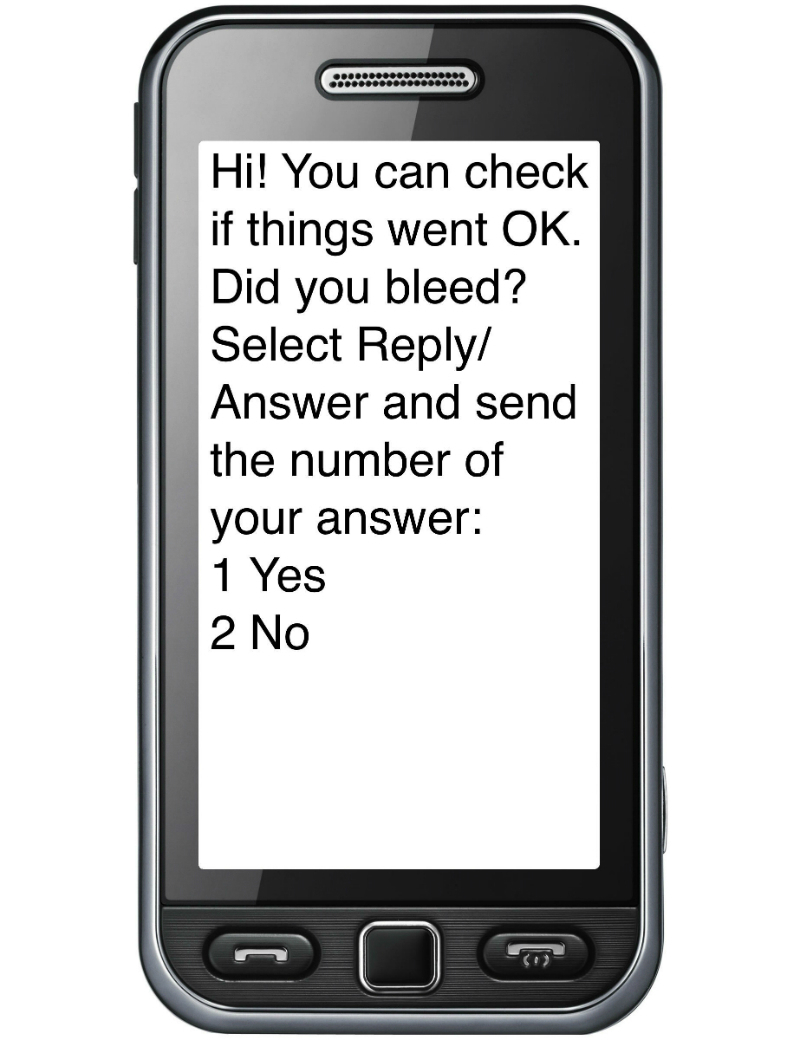
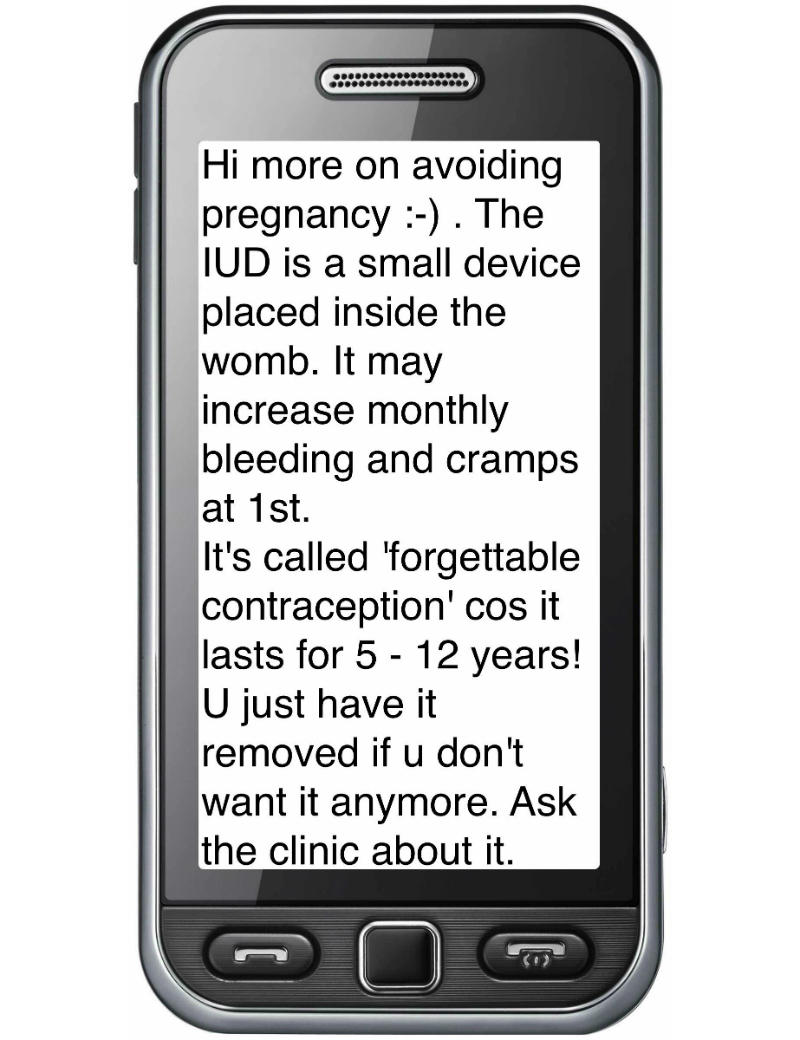
Methods: Mobile phones were used in three ways in the study: (1) coaching women through medical abortion using short message service (SMS; text messages); (2) a questionnaire to assess abortion completion via unstructured supplementary service data (USSD, a protocol used by GSM mobile telephones that allows the user to interact with a server via text-based menus) and the South African mobile instant message and social networking application Mxit; and (3) family planning information via SMS, mobisite and Mxit. A needs and context assessment was done to learn about women's experiences undergoing medical abortion and their use of mobile phones. After development, the mobile interventions were piloted. Recruitment was done by field workers at the clinics. In the RCT, women were interviewed at baseline and exit. Computer logs were also analyzed. All study participants received standard of care at the clinics.
Results: In the RCT, 234 women were randomized to the intervention group. Eight did not receive the intervention due to invalid numbers, mis-registration, system failure, or opt-out, leaving 226 participants receiving the full intervention. Of the 226, 190 returned and were interviewed at their clinic follow-up visit. The SMSs were highly acceptable, with 97.9% (186/190) saying that the SMSs helped them through the medical abortion. In terms of mobile phone privacy, 86.3% (202/234) said that it was not likely or possible that someone would see SMSs on their phone, although at exit, 20% (38/190) indicated that they had worried about phone privacy. Having been given training at baseline and subsequently asked via SMS to complete the self-assessment questionnaire, 90.3% (204/226) attempted it, and of those, 86.3% (176/204) reached an endpoint of the questionnaire. For the family planning information, a preference for SMS was indicated by study clients, although the publicly available Mxit/mobisite was heavily used (813,375 pages were viewed) over the study duration.
Conclusions: SMS provided a good medium for timed, "push" information that guided and supported women through medical abortion. Women were able to perform a self-assessment questionnaire via mobile phones if provided training and prompted by SMS. Phone privacy needs to be protected in similar settings. This study may contribute to the successful expansion of medical abortion provision aided by mobile phones.
Trial registration: Pan African Clinical Trials Registry (PACTR): PACTR201302000427144; http://www.pactr.org/ATMWeb/appmanager/atm/atmregistry?dar=true&tNo=PACTR201302000427144 (Archived by WebCite at http://www.webcitation.org/6N0fnZfzm).
Keywords: SMS; USSD; mHealth; medical abortion; mobisite; telemedicine.
Conflict of interest statement
Conflicts of Interest: Conflicts of Interest: None declared.
Figures
References
-
- Blanchard K, Cooper D, Dickson K, Cullingworth L, Mavimbela N, von Mollendorf C, van Bogaert LJ, Winikoff B. A comparison of women's, providers' and ultrasound assessments of pregnancy duration among termination of pregnancy clients in South Africa. BJOG. 2007 May;114(5):569–75. doi: 10.1111/j.1471-0528.2007.01293.x. - DOI - PubMed
-
- Blanchard K, Schaffer K, McLeod S, Winikoff B. Medication abortion in the private sector in South Africa. Eur J Contracept Reprod Health Care. 2006 Dec;11(4):285–90. - PubMed
-
- Kawonga M, Blanchard K, Cooper D, Cullingworth L, Dickson K, Harrison T, von Mollendorf C, Winikoff B. Integrating medical abortion into safe abortion services: experience from three pilot sites in South Africa. J Fam Plann Reprod Health Care. 2008 Jul;34(3):159–64. doi: 10.1783/147118908784734846. http://jfprhc.bmj.com/cgi/pmidlookup?view=long&pmid=18577314 - DOI - PubMed
-
- Hassoun D. Medical Abortion Technologies of 21st Century. ICMA/IPAS African Meeting on Medical Abortion; 11-13 March, 2009; Johannesburg, South Africa. 2009. Mar 11-13, http://www.medicalabortionconsortium.org/uploads/file/D_HASSOUN%202009%2...
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
