

Breast imaging findings in haematological malignancies
- PMID: 25099481
- PMCID: PMC4263805
- DOI: 10.1007/s13244-014-0344-2
Breast imaging findings in haematological malignancies
Abstract
Objectives: The objectives of this article are to review and illustrate the imaging appearances of haematological malignancies in the breast.
Methods: With Institutional Review Board approval, a search of the surgical pathology records from 1st January 2000 to 1st July 2012 was performed for haematological malignancies.
Results: Forty-eight cases of haematological malignancies (42 women and 6 men) were identified with imaging available for review: 39 cases of breast lymphoma, 6 cases of chronic lymphocytic leukaemia, 2 cases of acute leukaemia and 1 case of known multiple myeloma.
Conclusions: Breast manifestations of haematological malignancies are rare. They can have a variable appearance at imaging and can mimic primary breast carcinoma. In the setting of suspicious breast imaging findings, pathological diagnosis of haematological malignancy is concordant. Correlation with a clinical history of prior haematological malignancy can be helpful in suggesting the diagnosis and help prevent unnecessary surgical treatment.
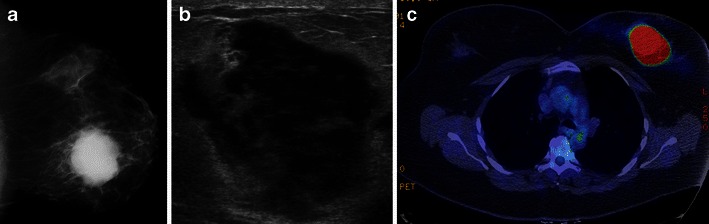
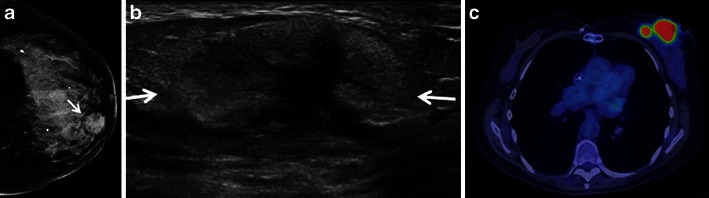
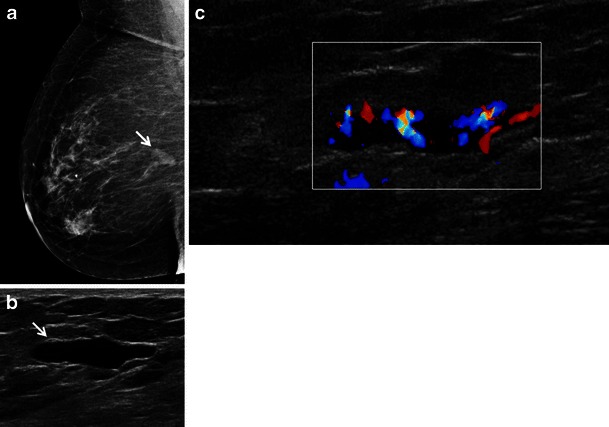
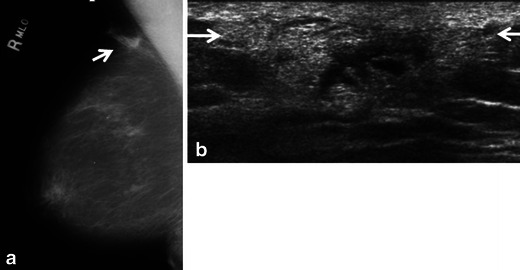
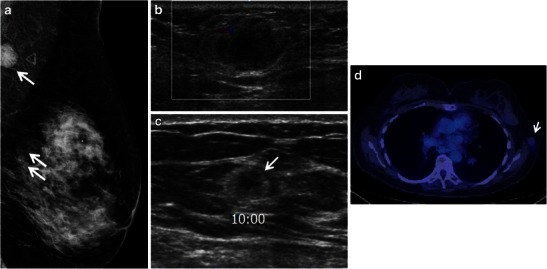
Teaching points: • Breast haematological malignancies are rare but the imaging appearances can mimic breast carcinoma. • Breast lymphoma, most often B-cell non-Hodgkin lymphoma, may be primary or due to secondary disease. • At ultrasound, haematological malignancies may present as a heterogeneous or predominantly echogenic mass. • Haematological malignancies show intense activity on PET/CT except myeloma which has low FDG uptake.
Figures



References
-
- American Cancer Society . Cancer facts & figures 2013. Atlanta: American Cancer Society; 2013.
LinkOut - more resources
Full Text Sources
Other Literature Sources
