

Methotrexate for induction of remission in refractory Crohn's disease
- PMID: 25099640
- PMCID: PMC7154581
- DOI: 10.1002/14651858.CD003459.pub4
Methotrexate for induction of remission in refractory Crohn's disease
Abstract
Background: Although corticosteroids are effective for induction of remission of Crohn's disease, many patients relapse when steroids are withdrawn or become steroid dependent. Furthermore, corticosteroids exhibit significant adverse effects. The success of methotrexate as a treatment for rheumatoid arthritis led to its evaluation in patients with refractory Crohn's disease. Methotrexate has been studied for induction of remission of refractory Crohn's disease and has become the principal alternative to azathioprine or 6-mercaptopurine therapy. This systematic review is an update of previously published Cochrane reviews.
Objectives: The primary objective was to assess the efficacy and safety of methotrexate for induction of remission in patients with active Crohn's disease in the presence or absence of concomitant steroid therapy.
Search methods: We searched MEDLINE, EMBASE, CENTRAL and the Cochrane IBD/FBD group specialized register from inception to June 9, 2014 for relevant studies. Conference proceedings and reference lists were also searched to identify additional studies.
Selection criteria: Randomized controlled trials of methotrexate compared to placebo or an active comparator for treatment of active refractory Crohn's disease in adult patients (> 17 years) were considered for inclusion.
Data collection and analysis: The primary outcome was failure to enter remission and withdraw from steroids. Secondary outcomes included adverse events, withdrawal due to adverse events, serious adverse events and quality of life. We calculated the relative risk (RR) and 95% confidence intervals (95% CI) for each outcome. Data were analyzed on an intention-to-treat basis. The Cochrane risk of bias tool was used to assess the methodological quality of included studies. The GRADE approach was used to assess the overall quality of evidence supporting the primary outcome.
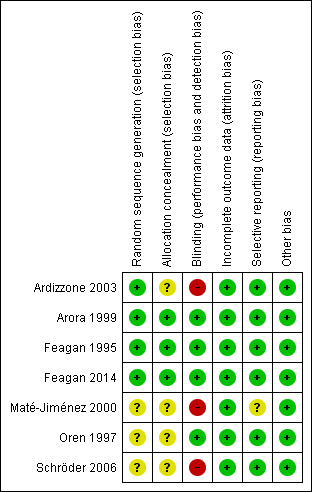
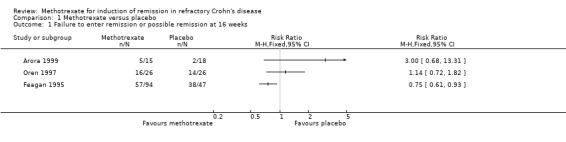
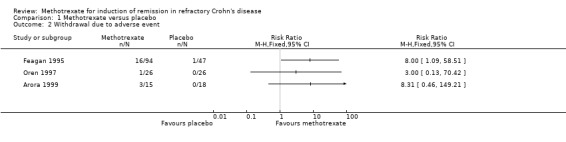
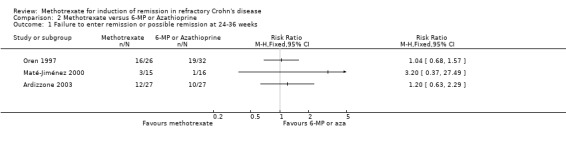
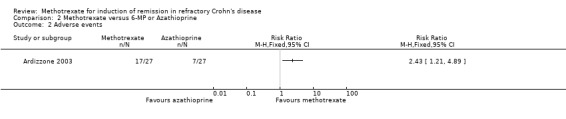
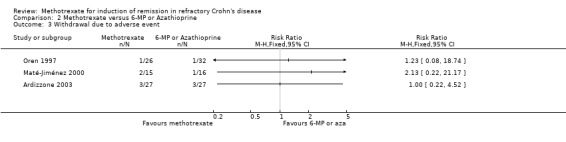
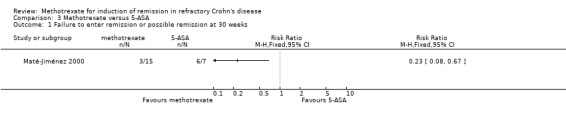
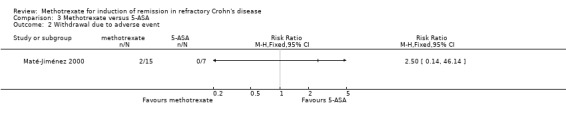
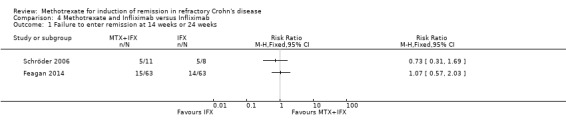
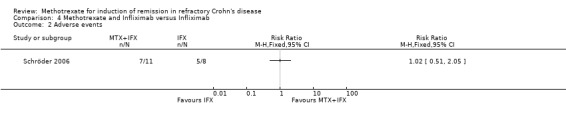
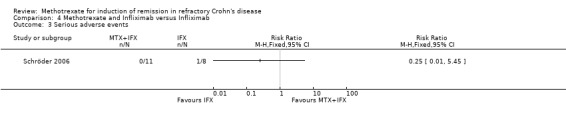
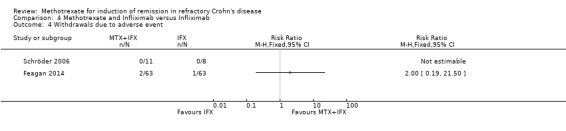
Main results: Seven studies (495 patients) were included. Four studies were rated as low risk of bias. Three studies were rated as high risk of bias due to open label or single-blind designs. The seven studies differed with respect to participants, intervention, and outcomes to the extent that meta-analysis was considered to be inappropriate. GRADE analyses indicated that the quality of evidence was very low to low for most outcomes due to sparse data and inadequate blinding. Three small studies which employed low dose oral methotrexate showed no statistically significant difference in failure to induce remission between methotrexate and placebo or between methotrexate and 6-mercaptopurine. For the study using 15 mg/week of oral methotrexate 33% (5/15) of methotrexate patients failed to enter remission compared to 11% (2/18) of placebo patients (RR 3.00, 95% CI 0.68 to 13.31). For the study using 12.5 mg/week of oral methotrexate 81% (21/26) of methotrexate patients failed to enter remission compared to 77% (20/26) of placebo patients (RR 1.05, 95% CI 0.79 to 1.39). This study also had an active comparator arm, 81% (21/26) of methotrexate patients failed to enter remission compared to 59% (19/32) of 6-mercaptopurine patients (RR 1.36, 95% CI 0.97 to 1.92). For the active comparator study using 15 mg/week oral methotrexate, 20% (3/15) of methotrexate patients failed to enter remission compared to 6% of 6-mercaptopurine patients (RR 3.20, 95% CI 0.37 to 27.49). This study also had a 5-ASA arm and found that methotrexate patients were significantly more likely to enter remission than 5-ASA patients. Twenty per cent (3/15) of methotrexate patients failed to enter remission compared to 86% (6/7) of 5-ASA patients (RR 0.23, 95% CI 0.08 to 0.67). One small study which used a higher dose of intravenous or oral methotrexate (25 mg/week) showed no statistically significant difference between methotrexate and azathioprine. Forty-four per cent (12/27) of methotrexate patients failed to enter remission compared to 37% of azathioprine patients (RR 1.20, 95% CI 0.63 to 2.29). Two studies found no statistically significant difference in failure to enter remission between the combination of infliximab and methotrexate and infliximab monotherapy. One small study utilized intravenous methotrexate (20 mg/week) for 5 weeks and then switched to oral (20 mg/week). Forty-five per cent (5/11) of patients in the combination group failed to enter remission compared to 62% of infliximab patients (RR 0.73, 95% CI 0.31 to 1.69). The other study assessing combination therapy utilized subcutaneous methotrexate (maximum dose 25 mg/week). Twenty-four per cent (15/63) of patients in the combination group failed to enter remission compared to 22% (14/63) of infliximab patients (RR 1.07, 95% CI 0.57 to 2.03). A large placebo-controlled study which employed a high dose of methotrexate intramuscularly showed a statistically significant benefit relative to placebo. Sixty-one per cent of methotrexate patients failed to enter remission compared to 81% of placebo patients (RR 0.75, 95% CI 0.61 to 0.93; number needed to treat, NNT=5). Withdrawals due to adverse events were significantly more common in methotrexate patients than placebo in this study. Seventeen per cent of methotrexate patients withdrew due to adverse events compared to 2% of placebo patients (RR 8.00, 95% CI 1.09 to 58.51). The incidence of adverse events was significantly more common in methotrexate patients (63%, 17/27) than azathioprine patients (26%, 7/27) in one small study (RR 2.42, 95% CI 1.21 to 4.89). No other statistically significant differences in adverse events, withdrawals due to adverse events or serious adverse events were reported in any of the other placebo-controlled or active comparator studies. Common adverse events included nausea and vomiting, abdominal pain, diarrhea, skin rash and headache.
Authors' conclusions: There is evidence from a single large randomized trial which suggests that intramuscular methotrexate (25 mg/week) provides a benefit for induction of remission and complete withdrawal from steroids in patients with refractory Crohn's disease. Lower dose oral methotrexate does not appear to provide any significant benefit relative to placebo or active comparator. However, these trials were small and further studies of oral methotrexate may be justified. Comparative studies of methotrexate to drugs such as azathioprine or 6-mercaptopurine would require the randomization of large numbers of patients. The addition of methotrexate to infliximab therapy does not appear to provide any additional benefit over infliximab monotherapy. However these studies were relatively small and further research is needed to determine the role of methotrexate when used in conjunction with infliximab or other biological therapies.
Conflict of interest statement
Brian Feagan and John WD McDonald are authors of two manuscripts that were included in this review. Brian Feagan has received fee(s) from Abbott/AbbVie, Amgen, Astra Zeneca, Avaxia Biologics Inc., Bristol‐Myers Squibb, Celgene, Centocor Inc., Elan/Biogen, Ferring, JnJ/Janssen, Merck, Novartis, Novonordisk, Pfizer, Prometheus Laboratories, Protagonist, Salix Pharma, Takeda, Teva, Tillotts Pharma AG, UCB Pharma for Board membership; fee(s) from Abbott/AbbVie, Actogenix, Albireo Pharma, Amgen, Astra Zeneca, Avaxia Biologics Inc., Axcan, Baxter Healthcare Corp., Boehringer‐Ingelheim, Bristol‐Myers Squibb, Calypso Biotech, Celgene, Elan/Biogen, EnGene, Ferring Pharma, Roche/Genentech, GiCare Pharma, Gilead, Given Imaging Inc., GSK, Ironwood Pharma, Janssen Biotech (Centocor), JnJ/Janssen, Kyowa Kakko Kirin Co Ltd., Lexicon, Lilly, Merck, Millennium, Nektar, Novonordisk, Pfizer, Prometheus Therapeutics and Diagnostics, Protagonist, Receptos, Salix Pharma, Serono, Shire, Sigmoid Pharma, Synergy Pharma Inc., Takeda, Teva Pharma, Tillotts, UCB Pharma, Vertex Pharma, Warner‐Chilcott, Wyeth, Zealand, and Zyngenia for consultancy; and lecture fee(s) from: Abbott/AbbVie, JnJ/Janssen, Takeda, Warner‐Chilcott, and UCB Pharma. All of these activities are outside the submitted work.
The other authors have no known declarations of interest.
Figures

Update of
-
Methotrexate for induction of remission in refractory Crohn's disease.Cochrane Database Syst Rev. 2012 Dec 12;12:CD003459. doi: 10.1002/14651858.CD003459.pub3. Cochrane Database Syst Rev. 2012. Update in: Cochrane Database Syst Rev. 2014 Aug 06;(8):CD003459. doi: 10.1002/14651858.CD003459.pub4. PMID: 23235598 Updated.
References
References to studies included in this review
Ardizzone 2003 {published data only}
-
- Ardizzone S, Bollani S, Manzionna G, Imbesi V, Colombo E, Bianchi Porro G. Comparison between methotrexate and azathioprine in the treatment of chronic active Crohn's disease: a randomised, investigator‐blind study. Digestive and Liver Disease 2003;35:619‐27. [PUBMED: 14563183] - PubMed
-
- Ardizzone S, Bollani S, Manzionna G, Molteni P, Bareggi E, Bianchi Porro G. Controlled trial comparing intravenous methotrexate and oral azathioprine for chronic active Crohn's disease: preliminary report. Gastroenterology 1999;116(4 Part 2):A662‐3.
-
- Bianchi Porro G, Ardizzone S, Bollani S, Duca A, Manzionna G, Molteni P. Controlled trial comparing intravenous methotrexate and oral azathioprine for chronic active Crohn's disease: preliminary report. Gut 1982;23:295.
Arora 1999 {published data only}
-
- Arora S, Katkov W, Cooley J, Kemp JA, Johnston DE, Schapiro RH, et al. Methotrexate in Crohn's disease: results of a randomized, double‐blind, placebo‐controlled trial. Hepatogastroenterology 1999;46(27):1724‐9. [PUBMED: 10430331] - PubMed
-
- Arora S, Katkov WN, Cooley J, Kemp A, Schapiro RH, Kelsey PB, et al. A double blind, randomized, placebo‐controlled trial of methotrexate in Crohn's disease. Gastroenterology 1992;102(4 Part 2):A591. - PubMed
Feagan 1995 {published data only}
-
- Feagan B. A multicentre trial of methotrexate (MTX) for chronically active Crohn's disease (CD). Gut 1994;35 Suppl 4:A121.
-
- Feagan BG, Rochon J, Fedorak RN, Irvine EJ, Wild G, Sutherland L, et al. Methotrexate for the treatment of Crohn's disease. The North American Crohn's Study Group Investigators. New England Journal of Medicine 1995;332:292‐7. [PUBMED: 7816064] - PubMed
-
- The North American Crohn's Study Group Investigators. A multicentre trial of methotrexate (MTX) treatment for chronically active Crohn's disease. Gastroenterology 1994;106(4 Part 2):A745.
Feagan 2014 {published data only}
-
- Feagan B, McDonald J, Panaccione R, Enns R, Bernstein C, Ponich T, et al. A randomized trial of methotrexate in combination with infliximab for the treatment of Crohn's disease. Gastroenterology 2008;135(1):294‐5.
-
- Feagan BG, McDonald JW, Panaccione R, Enns RA, Bernstein CN, Ponich TP, et al. Methotrexate in combination with infliximab is no more effective than infliximab alone in patients with Crohn’s disease. Gastroenterology 2014;146(3):681‐8. [PUBMED: 24269926] - PubMed
-
- Feagan BG, McDonald JWD, Panaccione R, Enns R, Bernstein CN, Ponich T, et al. A randomized trial of methotrexate in combination with infliximab for the treatment of Crohn's disease. United European Gastroenterology Week. Vienna, Austria, 2008.
Maté‐Jiménez 2000 {published data only}
-
- Hermida C, Cantero J, Moreno‐Otero R, Maté‐Jiménez J. Methotrexate and 6‐mercaptopurine in steroid‐dependent inflammatory bowel disease patients: a randomized controlled clinical trial. Gut 1999;45:A132.
-
- Maté‐Jiménez J, Hermida C, Cantero‐Perona J, Moreno‐Otero R. 6‐Mercaptopurine or methotrexate added to prednisone induces and maintains remission in steroid‐dependent inflammatory bowel disease. European Journal of Gastroenterology and Hepatology 2000;12:1227‐33. [PUBMED: 11111780] - PubMed
Oren 1997 {published data only}
-
- Oren R, Moshkowitz M, Odes S, Becker S, Keter D, Pomeranz I, et al. Methotrexate in chronic active Crohn's disease: a double‐blind, randomized, Israeli multicenter trial. American Journal of Gastroenterology 1997;92:2203‐9. [PUBMED: 1997381066] - PubMed
Schröder 2006 {published data only}
-
- Schröder O, Blumenstein I, Stein J. Combining infliximab with methotrexate for the induction and maintenance of remission in refractory Crohn's disease: a controlled pilot study. European Journal of Gastroenterology and Hepatology 2006;18(11):11‐6. [PUBMED: 16357613] - PubMed
References to studies excluded from this review
Clark 2009 {published data only}
-
- Clark L, Lightbody E, Morgan A, Gaya D, Winter J, Gillespie R, et al. The efficacy of long term intramuscular methotrexate in difficult to treat Crohn's disease. Gastroenterology 2009;136(5 Suppl 1):A659.
Domènech 2008 {published data only}
-
- Domènech E, Mañosa M, Navarro M, Masnou H, Garcia‐Planella E, Zabana Y, et al. Long‐term methotrexate for Crohn's disease: safety and efficacy in clinical practice. Journal of Clinical Gastroenterology 2008;42(4):395‐9. [PUBMED: 18277899] - PubMed
Egan 1999 {published data only}
-
- Egan LJ, Sandborn WJ, Leighton JA, Mays DC, Pike MG, Zinsmeister AR, et al. A randomized dose‐response and pharmacokinetic study of methotrexate for refractory inflammatory Crohn's disease and ulcerative colitis. Alimentary Pharmacology and Therapeutics 1999;13:1597‐604. [PUBMED: 10594394] - PubMed
-
- Egan LJ, Sandborn WJ, Tremaine WJ, Leighton JA, Mays DC, Pike MG, et al. A randomized, single‐blind, pharmacokinetic and doseresponse study of subcutaneous methotrexate, 15 and 25 mg/week, for refractory ulcerative colitis and Crohn's disease. Gastroenterology 1998;114(4 Pt 2):A227.
Feagan 2000 {published data only}
-
- Feagan BG, Fedorak RN, Irvine EJ, Wild G, Sutherland L, Steinhart AH, et al. A comparison of methotrexate with placebo for the maintenance of remission in Crohn's disease. North AmericanCrohn's Study Group Investigators. New England Journal of Medicine 2000;342(22):1627‐32. [PUBMED: 2000197470] - PubMed
Hayee 2005 {published data only}
-
- Hayee BH, Harris AW. Methotrexate for Crohn's disease: experience in a district general hospital. European Journal of Gastroenterology and Hepatology 2005;17(9):893‐8. [PUBMED: 16093864] - PubMed
Houben 1994 {published data only}
-
- Houben M, Wijk H, Driessen W, Spreeuwel J. Methotrexate as possible treatment of refractory chronic inflammatory bowel disease. Nederlands Tijdschrift Voor Geneeskunde 1992;138:2552‐6. [PUBMED: 7830804] - PubMed
Kurnik 2003 {published data only}
-
- Kurnik D, Loebstein R, Fishbein E, Almog S, Halkin H, Bar‐Meir S, et al. Bioavailability of oral vs. subcutaneous low‐dose methotrexate in patients with Crohn's disease. Alimentary Pharmacology and Therapeutics 2003;18(1):57‐63. [PUBMED: 12848626] - PubMed
Laharie 2011 {published data only}
-
- Laharie D, Reffet A, Belleannée G, Chabrun E, Subtil C, Razaire S, et al. Mucosal healing with methotrexate in Crohn's disease: a prospective comparative study with azathioprine and infliximab. Alimentary Pharmacology and Therapeutics 2011;33(6):714‐21. [PUBMED: 21235604] - PubMed
Lampen‐Smith 2011 {published data only}
-
- Lampen‐Smith A, Khan I, Claydon A. Methotrexate in patients with Crohn’s disease: a regional experience. Journal of Gastroenterology and Hepatology 2011;26:61‐2.
Lémann 2000 {published data only}
-
- Lémann M, Zenjari T, Bouhnik Y, Cosnes J, Mesnard B, Rambaud JC, et al. Methotrexate in Crohn's disease: long‐term efficacy and toxicity. American Journal of Gastroenterology 2000;95:1730‐4. [PUBMED: 10925976] - PubMed
Schröder 1996 {published data only}
-
- Schröder O, Stein J. Methotrexate in therapy of chronic inflammatory bowel diseases [Methotrexat (MTX) in der Therapie chronische‐entzundlicher Darmerkrankungen]. Zeitschrift fur Gastroenterologie 1996;34(7):457‐8. [PUBMED: 8928541] - PubMed
Suares 2012 {published data only}
-
- Suares NC, Hamlin PJ, Greer DP, Warren L, Clark T, Ford AC. Efficacy and tolerability of methotrexate therapy for refractory Crohn's disease: a large single‐centre experience. Alimentary Pharmacology and Therapeutics 2012;35(2):284‐91. [PUBMED: 22112005] - PubMed
Sun 2005 {published data only}
-
- Sun JH, Das KM. Low‐dose oral methotrexate for maintaining Crohn's disease remission: where we stand. Journal of Clinical Gastroenterology 2005;39(9):751‐6. [PUBMED: 16145336] - PubMed
Wilson 2013 {published data only}
-
- Wilson A, Patel V, Chande N, Ponich T, Urquhart B, Asher L, et al. Pharmacokinetic profiles for oral and subcutaneous methotrexate in patients with Crohn's disease. Alimentary Pharmacology and Therapeutics 2013;37(3):340‐5. [PUBMED: 23190184] - PubMed
Additional references
Balis 1988
-
- Balis FM, Mirro J Jr, Reaman GH, Evans WE, McCully C, Dehorty KM, et al. Pharmacokinetics of subcutaneous methotrexate. Journal of Clinical Oncology 1988;6(12):1882‐6. - PubMed
Baron 1993
-
- Baron TH, Truss CD, Elson CO. Low‐dose oral methotrexate in refractory inflammatory bowel disease. Digestive Diseases and Sciences 1993;38(10):1851‐6. - PubMed
Binder 1985
Brooks 1990
-
- Brooks PJ, Spruill WJ, Parish RC, Birchmore DA. Pharmacokinetics of methotrexate administered by intramuscular and subcutaneous injections in patients with rheumatoid arthritis. Arthritis and Rheumatism 1990;33(1):91‐4. - PubMed
Chande 2013
Egan 1999b
-
- Egan LJ, Sandborn WJ, Mays DC, Tremaine WJ, Fauq AH, Lipsky JJ. Systemic and intestinal pharmacokinetics of methotrexate in patients with inflammatory bowel disease. Clinical Pharmacology and Therapeutics 1999;65(1):29‐39. - PubMed
Griffith 2000
-
- Griffith SM, Fisher J, Clarke S, Montgomery B, Jones PW, Saklatvala J, et al. Do patients with rheumatoid arthritis established on methotrexate and folic acid 5 mg daily need to continue folic acid supplements long term?. Rheumatology 2000;39(10):1102‐9. - PubMed
Guyatt 2008
Harvey 1980
-
- Harvey RF, Bradshaw JM. A simple index of Crohn's‐disease activity. Lancet 1980;1(8167):514. - PubMed
Higgins 2011
-
- Higgins JPT, Altman DG, Sterne JAC (editors). Chapter 8: Assessing risk of bias in included studies. In: Higgins JPT, Green S editor(s). Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 (updated March 2011). The Cochrane Collaboration, 2011. Available from www.cochrane‐handbook.org.
Kozarek 1989
-
- Kozarek RA, Patterson DJ, Gelfand MD, Botoman VA, Ball TJ, Wilske KR. Methotrexate induces clinical and histologic remission in patients with refractory inflammatory bowel disease. Annals of Internal Medicine 1989;110(5):353‐6. - PubMed
Kremer 1994
-
- Kremer JM, Alarcon GS, Lightfoot RW Jr, Willkens RF, Furst DE, Williams HJ, et al. Methotrexate for rheumatoid arthritis: Suggested guidelines for monitoring liver toxicity. Arthritis and Rheumatism 1994;37(3):316‐28. - PubMed
Lorenzi 2000
-
- Lorenzi AR, Johnson AH, Gough A. Daily folate supplementation is adequate prophylaxis against methotrexate‐induced nausea and vomiting and avoids the need for expensive anti‐emetic prescription. Rheumatology 2000;39(7):812‐3. - PubMed
McDonald 2005
Schünemann 2011
-
- Schünemann HJ, Oxman AD, Vist GE, Higgins JPT, Deeks JJ, Glasziou P, et al. Chapter 12: Interpreting results and drawing conclusions. In: Higgins JPT, Green S editor(s). Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 (updated March 2011). The Cochrane Collaboration, 2011. Available from www.cochrane‐handbook.org.
References to other published versions of this review
Alfadhli 2004
-
- Alfadhli AAF, McDonald JWD, Feagan BG. Methotrexate for induction of remission in refractory Crohn’s disease. Cochrane Database of Systematic Reviews 2004, Issue 4. [DOI: 10.1002/14651858.CD003459.pub2] - DOI
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical