

Effect of telehealth on glycaemic control: analysis of patients with type 2 diabetes in the Whole Systems Demonstrator cluster randomised trial
- PMID: 25100190
- PMCID: PMC4128403
- DOI: 10.1186/1472-6963-14-334
Effect of telehealth on glycaemic control: analysis of patients with type 2 diabetes in the Whole Systems Demonstrator cluster randomised trial
Abstract
Background: The Whole Systems Demonstrator was a large, pragmatic, cluster randomised trial that compared telehealth with usual care among 3,230 patients with long-term conditions in three areas of England. Telehealth involved the regular transmission of physiological information such as blood glucose to health professionals working remotely. We examined whether telehealth led to changes in glycosylated haemoglobin (HbA1c) among the subset of patients with type 2 diabetes.
Methods: The general practice electronic medical record was used as the source of information on HbA1c. Effects on HbA1c were assessed using a repeated measures model that included all HbA1c readings recorded during the 12-month trial period, and adjusted for differences in HbA1c readings recorded before recruitment. Secondary analysis averaged multiple HbA1c readings recorded for each individual during the trial period.
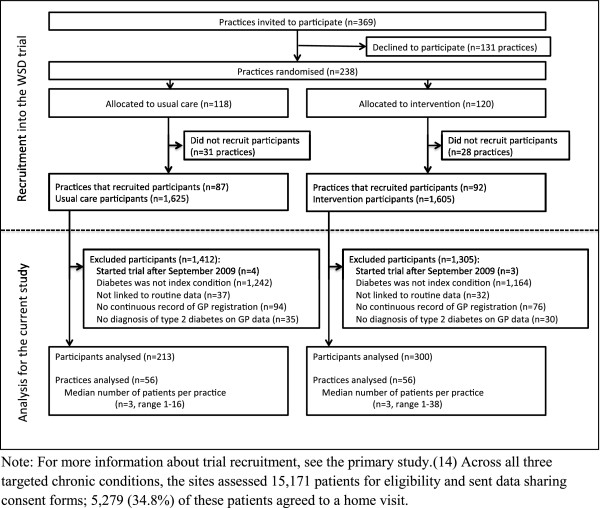
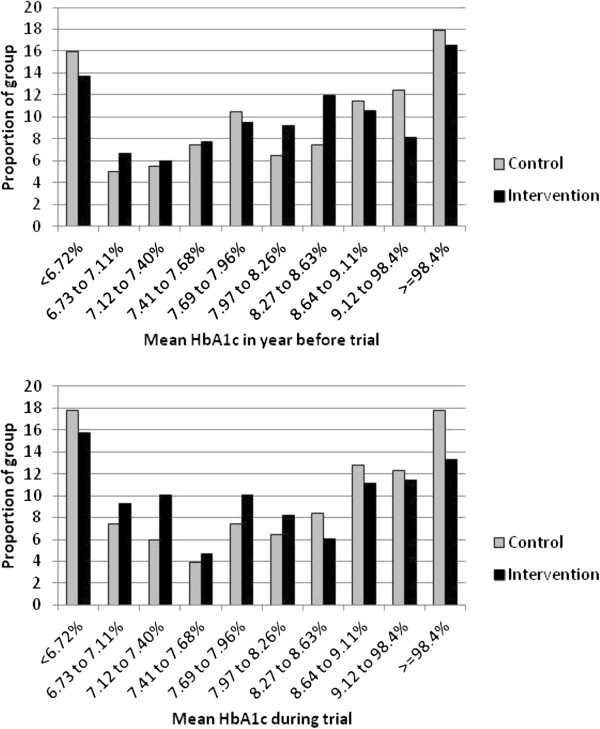
Results: 513 of the 3,230 participants were identified as having type 2 diabetes and thus were included in the study. Telehealth was associated with lower HbA1c than usual care during the trial period (difference 0.21% or 2.3 mmol/mol, 95% CI, 0.04% to 0.38%, p = 0.013). Among the 457 patients in the secondary analysis, mean HbA1c showed little change for controls following recruitment, but fell for intervention patients from 8.38% to 8.15% (68 to 66 mmol/mol). A higher proportion of intervention patients than controls had HbA1c below the 7.5% (58 mmol/mol) threshold that was targeted by general practices (30.4% vs. 38.0%). This difference, however, did not quite reach statistical significance (adjusted odds ratio 1.63, 95% CI, 0.99 to 2.68, p = 0.053).
Conclusions: Telehealth modestly improved glycaemic control in patients with type 2 diabetes over 12 months. The scale of the improvements is consistent with previous meta-analyses, but was relatively modest and seems unlikely to produce significant patient benefit.
Trial registration number: International Standard Randomized Controlled Trial Number Register ISRCTN43002091.
Figures
References
-
- Bardsley M, Steventon A, Smith J, Dixon J. Evaluating Integrated and Community-Based Care: How Do We Know What Works? London: Nuffield Trust; 2013.
-
- Inzucchi SE, Bergenstal RM, Buse JB, Diamant M, Ferrannini E, Nauck M, Peters AL, Tsapas A, Wender R, Matthews DR. Management of hyperglycemia in type 2 diabetes: a patient-centered approach: position statement of the American Diabetes Association (ADA) and the European Association for the Study of Diabetes (EASD) Diabetes Care. 2012;14:1364–1379. - PMC - PubMed
-
- Stone MA, Charpentier G, Doggen K, Kuss O, Lindblad U, Kellner C, Nolan J, Pazderska A, Rutten G, Trento M, Khunti K. Quality of care of people with type 2 diabetes in eight European Countries: findings from the Guideline Adherence to Enhance Care (GUIDANCE) study. Diabetes Care. 2013;14:2628–2638. - PMC - PubMed
-
- Clar C, Barnard K, Cummins E, Royle P, Waugh N. Self-monitoring of blood glucose in type 2 diabetes: systematic review. Health Technol Assess. 2010;14:1–140. - PubMed
-
- Kempf K, Tankova T, Martin S. ROSSO-in-praxi-international: long-term effects of self-monitoring of blood glucose on glucometabolic control in patients with type 2 diabetes mellitus not treated with insulin. Diabetes Technol Ther. 2013;14:89–96. - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
