

Serum iron concentration, but not hemoglobin, correlates with TIMI risk score and 6-month left ventricular performance after primary angioplasty for acute myocardial infarction
- PMID: 25100442
- PMCID: PMC4123974
- DOI: 10.1371/journal.pone.0104495
Serum iron concentration, but not hemoglobin, correlates with TIMI risk score and 6-month left ventricular performance after primary angioplasty for acute myocardial infarction
Abstract
Objective: Anemia is associated with high mortality and poor prognosis after acute coronary syndrome (ACS). Increased red cell distribution width (RDW) is a strong independent predictor for adverse outcomes in ACS. The common underlying mechanism for anemia and increased RDW value is iron deficiency. It is not clear whether serum iron deficiency without anemia affects left ventricular (LV) performance after primary angioplasty for acute myocardial infarction (AMI). We investigated the prognostic value of serum iron concentration on LV ejection fraction (EF) at 6 months and its relationship to thrombolysis in myocardial infarction (TIMI) risk score in post MI patients.
Methods: We recruited 55 patients who were scheduled to undergo primary coronary balloon angioplasty after AMI and 54 age- and sex-matched volunteers. Serum iron concentration and interleukin-6 levels were measured before primary angioplasty. LVEF was measured by echocardiography at baseline and after 6 months. TIMI risk score was calculated for risk stratification.
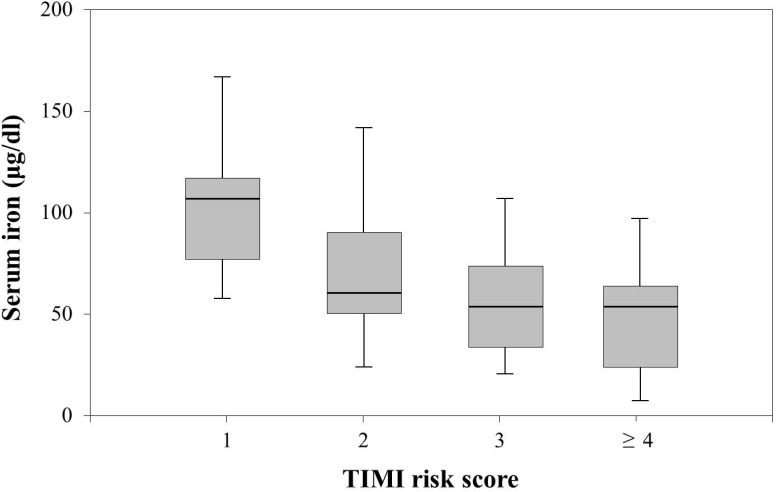
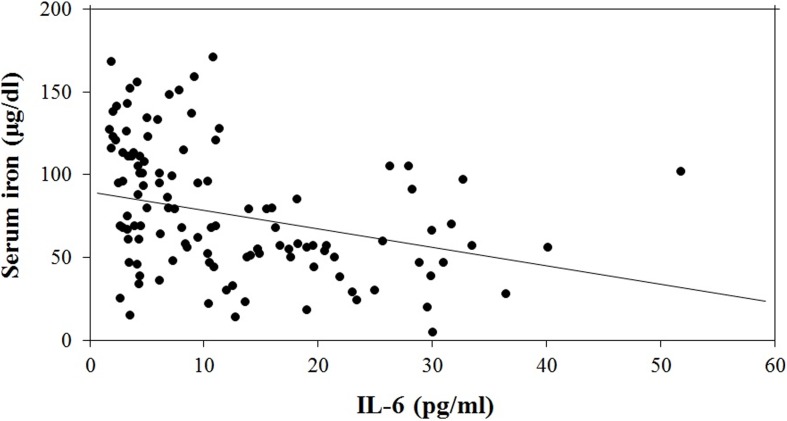
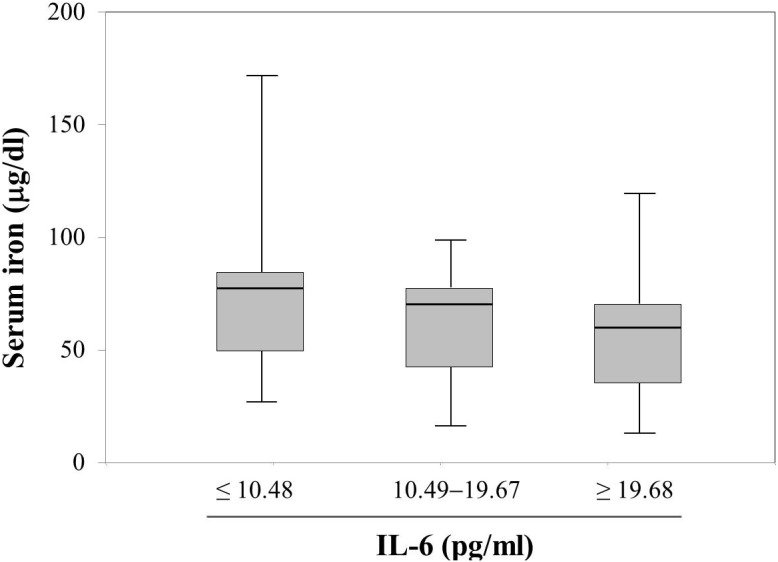
Results: Serum iron concentration was significantly lower in those in whom LVEF had not improved ≥ 10% from baseline (52.7 ± 24.1 versus 80.8 ± 50.8 µg/dl, P = 0.016) regardless of hemoglobin level, and was significantly lower in the AMI group than in the control group (62.5 ± 37.7 versus 103.0 ± 38.1 µg/dl, P<0.001). Trend analysis revealed that serum iron concentration decreased as TIMI risk score increased (P = 0.002). In addition, lower serum iron concentrations were associated with higher levels of inflammatory markers. Multiple linear regression showed that baseline serum iron concentration can predict LV systolic function 6 months after primary angioplasty for AMI even after adjusting for traditional prognostic factors.
Conclusion: Hypoferremia is not only a marker of inflammation but also a potential prognostic factor for LV systolic function after revascularization therapy for AMI, and may be a novel biomarker for therapeutic intervention.
Conflict of interest statement
Figures
References
-
- Anker SD, Comin Colet J, Filippatos G, Willenheimer R, Dickstein K, et al. (2009) Ferric carboxymaltose in patients with heart failure and iron deficiency. New England Journal of Medicine 361: 2436–2448. - PubMed
-
- Maeder MT, Khammy O, dos Remedios C, Kaye DM (2011) Myocardial and Systemic Iron Depletion in Heart FailureImplications for Anemia Accompanying Heart Failure. Journal of the American College of Cardiology 58: 474–480. - PubMed
-
- McMurray J, Ponikowski P (2011) Heart FailureNot Enough Pump Iron? Journal of the American College of Cardiology 58: 481–482. - PubMed
-
- Simel DL, DeLong ER, Feussner JR, Weinberg JB, Crawford J (1988) Erythrocyte anisocytosis: visual inspection of blood films vs automated analysis of red blood cell distribution width. Archives of internal medicine 148: 822–824. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
