

Optimizing human apyrase to treat arterial thrombosis and limit reperfusion injury without increasing bleeding risk
- PMID: 25100739
- PMCID: PMC4291186
- DOI: 10.1126/scitranslmed.3009246
Optimizing human apyrase to treat arterial thrombosis and limit reperfusion injury without increasing bleeding risk
Abstract
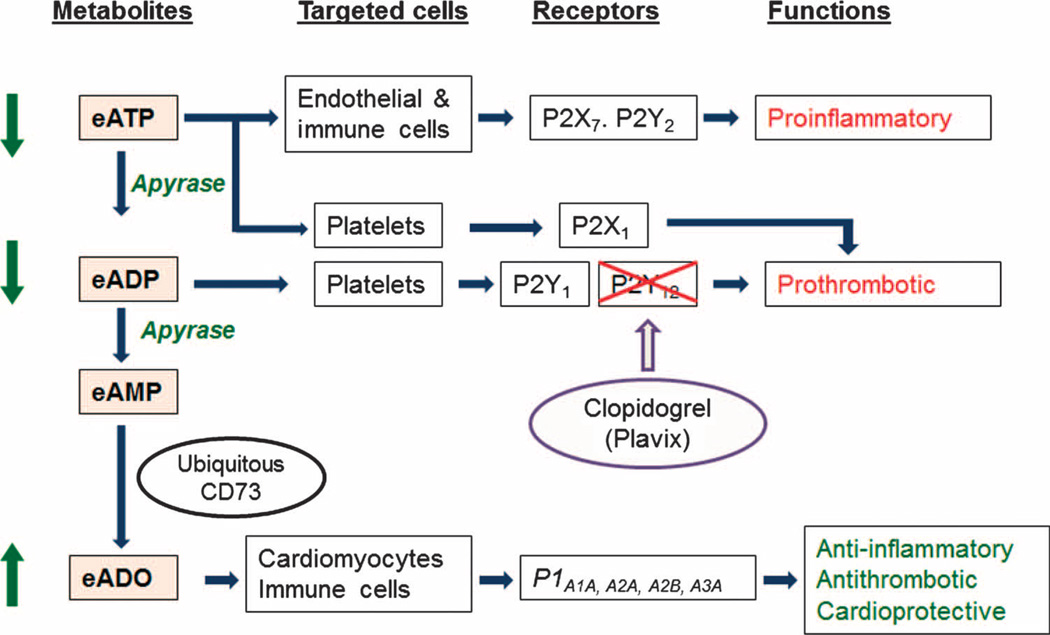
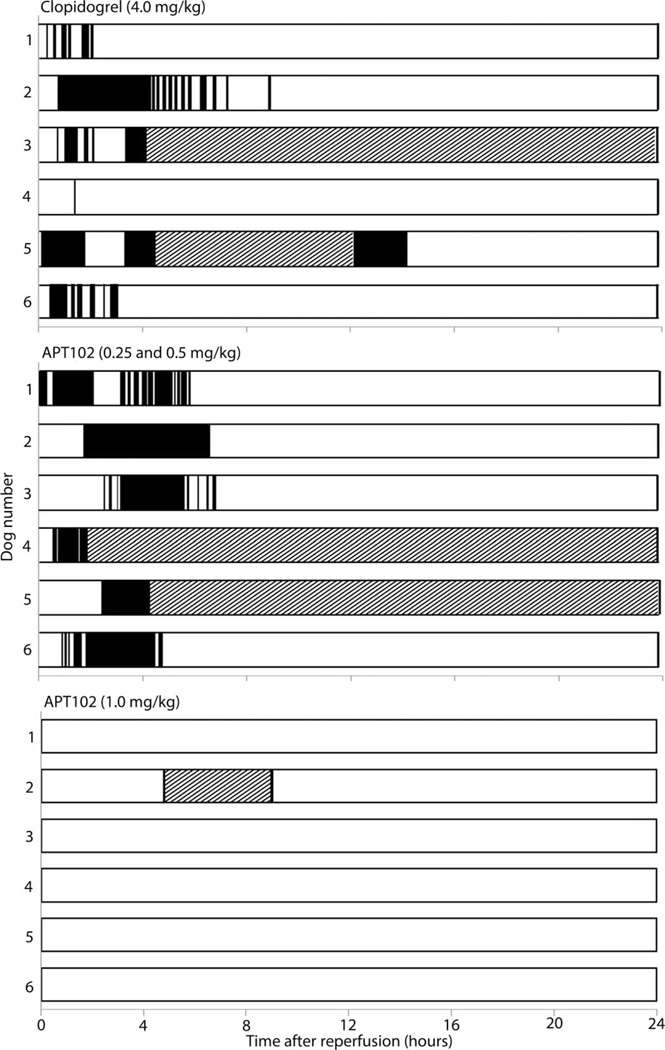
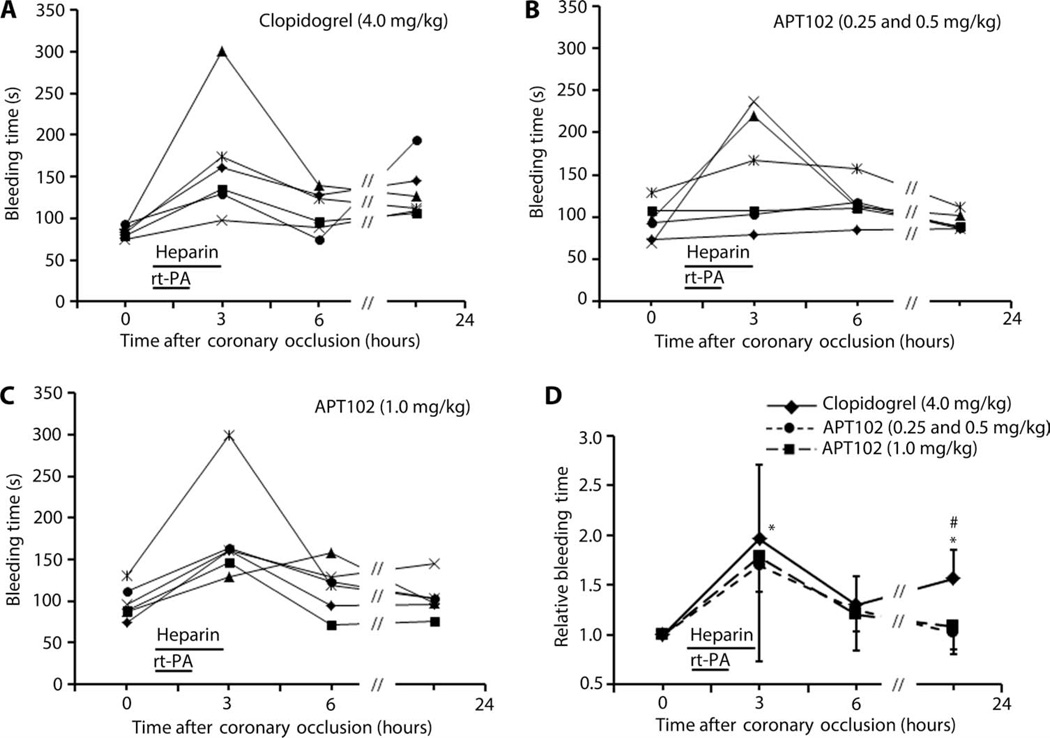
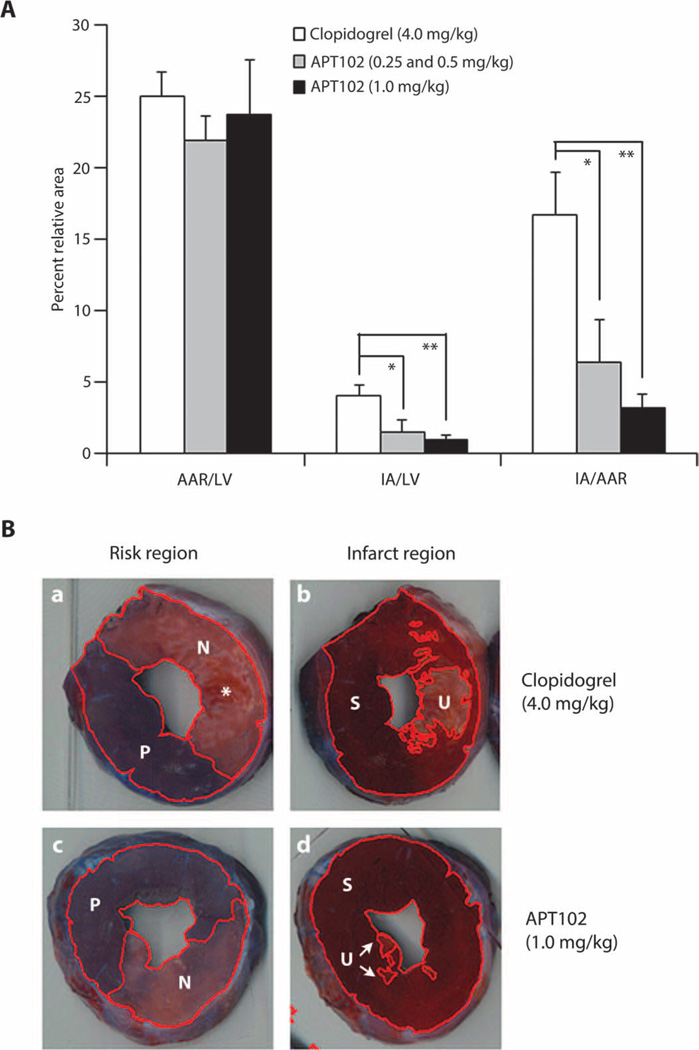
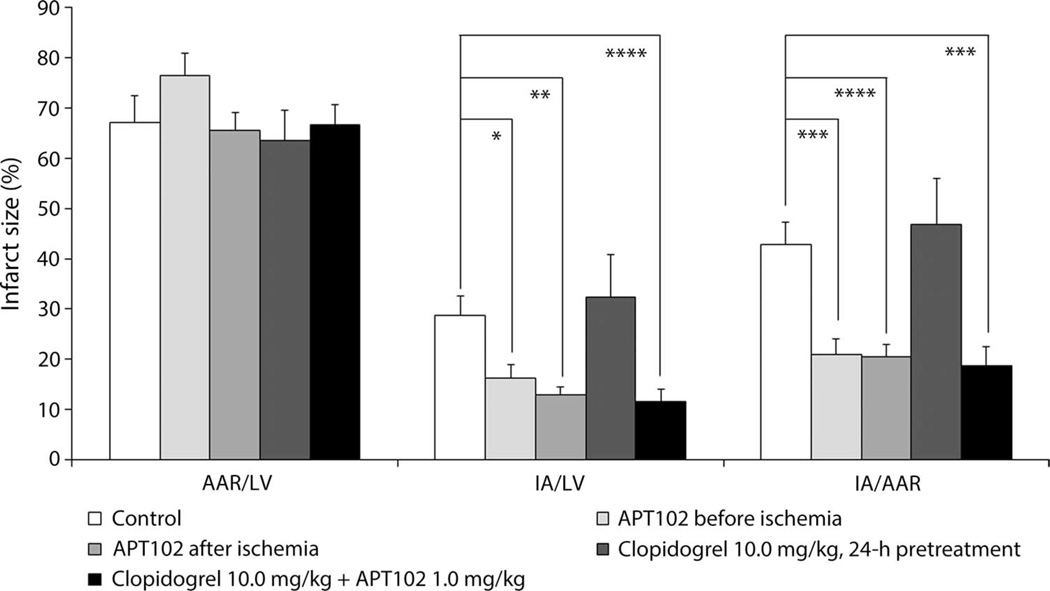
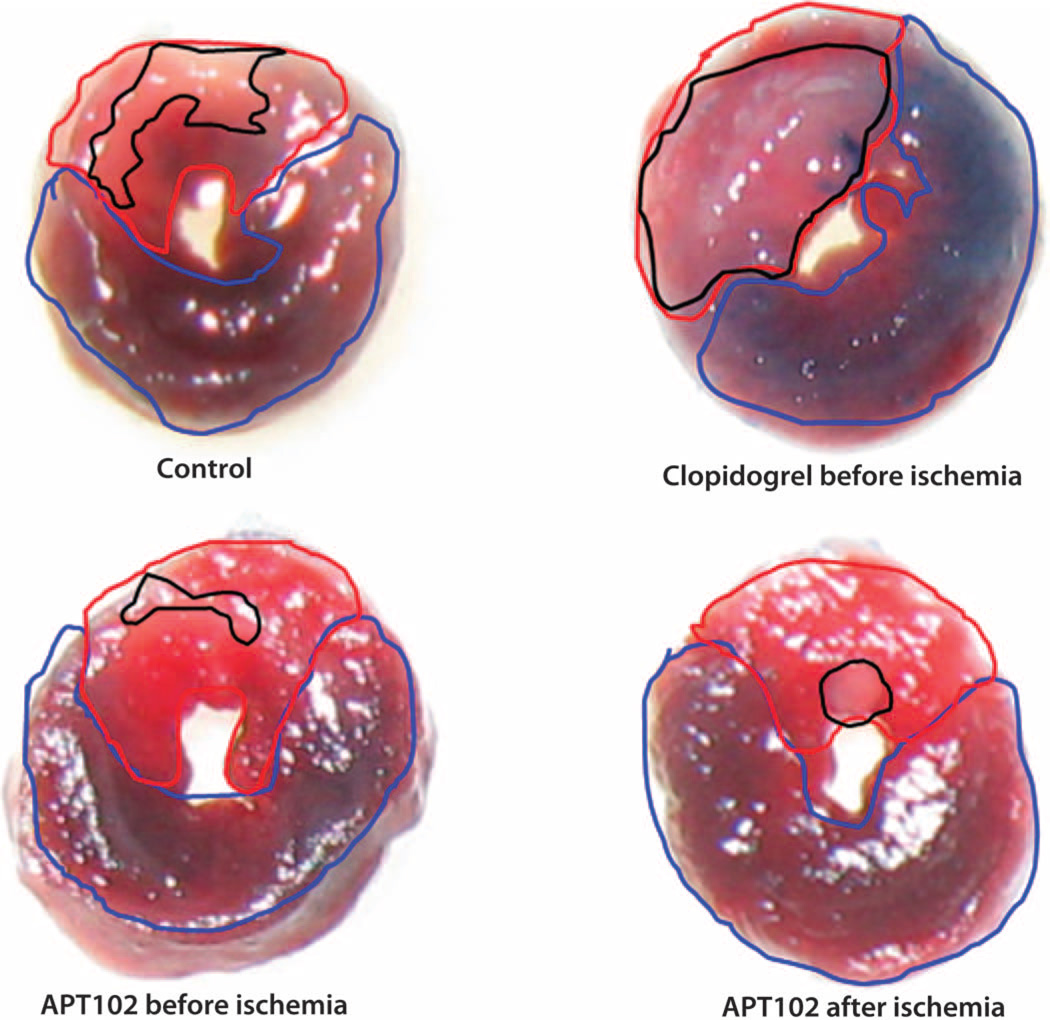
In patients with acute myocardial infarction undergoing reperfusion therapy to restore blood flow through blocked arteries, simultaneous inhibition of platelet P2Y12 receptors with the current standard of care neither completely prevents recurrent thrombosis nor provides satisfactory protection against reperfusion injury. Additionally, these antiplatelet drugs increase the risk of bleeding. To devise a different strategy, we engineered and optimized the apyrase activity of human nucleoside triphosphate diphosphohydrolase-3 (CD39L3) to enhance scavenging of extracellular adenosine diphosphate, a predominant ligand of P2Y12 receptors. The resulting recombinant protein, APT102, exhibited greater than four times higher adenosine diphosphatase activity and a 50 times longer plasma half-life than did native apyrase. Treatment with APT102 before coronary fibrinolysis with intravenous recombinant human tissue-type plasminogen activator in conscious dogs completely prevented thrombotic reocclusion and significantly decreased infarction size by 81% without increasing bleeding time. In contrast, clopidogrel did not prevent coronary reocclusion and increased bleeding time. In a murine model of myocardial reperfusion injury caused by transient coronary artery occlusion, APT102 also decreased infarct size by 51%, whereas clopidogrel was not effective. These preclinical data suggest that APT102 should be tested for its ability to safely and effectively maximize the benefits of myocardial reperfusion therapy in patients with arterial thrombosis.
Copyright © 2014, American Association for the Advancement of Science.
Figures
Comment in
-
Cardiovascular drugs: Engineered apyrase averts clot formation.Nat Rev Drug Discov. 2014 Oct;13(10):724-5. doi: 10.1038/nrd4444. Epub 2014 Sep 19. Nat Rev Drug Discov. 2014. PMID: 25233997 No abstract available.
References
-
- Go AS, Mozaffarian D, Roger VL, Benjamin EJ, Berry JD, Borden WB, Bravata DM, Dai S, Ford ES, Fox CS, Franco S, Fullerton HJ, Gillespie C, Hailpern SM, Heit JA, Howard VJ, Huffman MD, Kissela BM, Kittner SJ, Lackland DT, Lichtman JH, Lisabeth LD, Magid D, Marcus GM, Marelli A, Matchar DB, McGuire DK, Mohler ER, Moy CS, Mussolino ME, Nichol G, Paynter NP, Schreiner PJ, Sorlie PD, Stein J, Turan TN, Virani SS, Wong ND, Woo D, Turner MB. American Heart Association Statistics Committee and Stroke Statistics Subcommittee, Executive summary: Heart disease and stroke statistics—2013 update: A report from the American Heart Association. Circulation. 2013;127:143–152. - PubMed
-
- Kushner FG, Hand M, Smith SC, Jr, King SB, III, Anderson JL, Antman EM, Bailey SR, Bates ER, Blankenship JC, Casey DE, Green LA, Hochman JS, Jacobs AK, Krumholz HM, Morrison DA, Ornato JP, Pearle DL, Peterson ED, Sloan MA, Whitlow PL, Williams DO. American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines, 2009 Focused Updates: ACC/AHA Guidelines for the Management of Patients With ST-Elevation Myocardial Infarction (updating the 2004 Guideline and 2007 Focused Update) and ACC/AHA/SCAI Guidelines on Percutaneous Coronary Intervention (updating the 2005 Guideline and 2007 Focused Update): A report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. Circulation. 2009;120:2271–2306. - PubMed
-
- Mason PJ, Jacobs AK, Freedman JE. Aspirin resistance and atherothrombotic disease. J. Am. Coll. Cardiol. 2005;46:986–993. - PubMed
-
- Wallentin L. P2Y12 inhibitors: Differences in properties and mechanisms of action and potential consequences for clinical use. Eur. Heart J. 2009;30:1964–1977. - PubMed
-
- Wiviott SD, Braunwald E, McCabe CH, Montalescot G, Ruzyllo W, Gottlieb S, Neumann FJ, Ardissino D, De Servi S, Murphy SA, Riesmeyer J, Weerakkody G, Gibson CM, Antman EM TRITON-TIMI 38 Investigators. Prasugrel versus clopidogrel in patients with acute coronary syndromes. N. Engl. J. Med. 2007;357:2001–2015. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
