

Nonsurgical or Surgical Treatment of ACL Injuries: Knee Function, Sports Participation, and Knee Reinjury: The Delaware-Oslo ACL Cohort Study
- PMID: 25100769
- PMCID: PMC4116562
- DOI: 10.2106/JBJS.M.01054
Nonsurgical or Surgical Treatment of ACL Injuries: Knee Function, Sports Participation, and Knee Reinjury: The Delaware-Oslo ACL Cohort Study
Abstract
Background: While there are many opinions about the expected knee function, sports participation, and risk of knee reinjury following nonsurgical treatment of injuries of the anterior cruciate ligament (ACL), there is a lack of knowledge about the clinical course following nonsurgical treatment compared with that after surgical treatment.
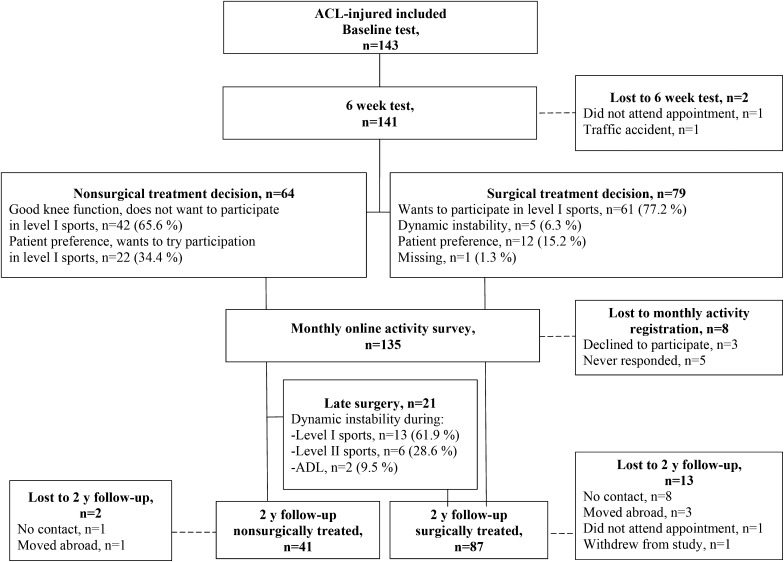
Methods: This prospective cohort study included 143 patients with an ACL injury. Isokinetic knee extension and flexion strength and patient-reported knee function as recorded on the International Knee Documentation Committee (IKDC) 2000 form were collected at baseline, six weeks, and two years. Sports participation was reported monthly for two years with use of an online activity survey. Knee reinjuries were reported at the follow-up evaluations and in a monthly online survey. Repeated analysis of variance (ANOVA), generalized estimating equation (GEE) models, and Cox regression analysis were used to analyze group differences in functional outcomes, sports participation, and knee reinjuries, respectively.
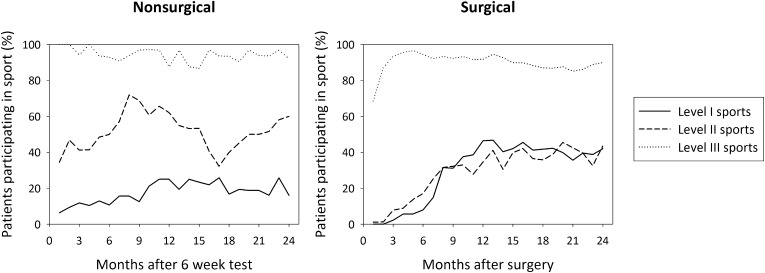
Results: The surgically treated patients (n = 100) were significantly younger, more likely to participate in level-I sports, and less likely to participate in level-II sports prior to injury than the nonsurgically treated patients (n = 43). There were no significant group-by-time effects on functional outcome. The crude analysis showed that surgically treated patients were more likely to sustain a knee reinjury and to participate in level-I sports in the second year of the follow-up period. After propensity score adjustment, these differences were nonsignificant; however, the nonsurgically treated patients were significantly more likely to participate in level-II sports during the first year of the follow-up period and in level-III sports over the two years. After two years, 30% of all patients had an extensor strength deficit, 31% had a flexor strength deficit, 20% had patient-reported knee function below the normal range, and 20% had experienced knee reinjury.
Conclusions: There were few differences between the clinical courses following nonsurgical and surgical treatment of ACL injury in this prospective cohort study. Regardless of treatment course, a considerable number of patients did not fully recover following the ACL injury, and future work should focus on improving the outcomes for these patients.
Level of evidence: Therapeutic Level II. See Instructions for Authors for a complete description of levels of evidence.
Copyright © 2014 by The Journal of Bone and Joint Surgery, Incorporated.
Figures
Comment in
- J Bone Joint Surg Am. 96(15):e133.
References
-
- Beynnon BD, Johnson RJ, Abate JA, Fleming BC, Nichols CE. Treatment of anterior cruciate ligament injuries, part I. Am J Sports Med. 2005October;33(10):1579-602 - PubMed
-
- Beaufils P, Hulet C, Dhénain M, Nizard R, Nourissat G, Pujol N. Clinical practice guidelines for the management of meniscal lesions and isolated lesions of the anterior cruciate ligament of the knee in adults. Orthop Traumatol Surg Res. 2009October;95(6):437-42 Epub 2009 Sep 10 - PubMed
-
- Roos H, Karlsson J. Anterior cruciate ligament instability and reconstruction. Review of current trends in treatment. Scand J Med Sci Sports. 1998December;8(6):426-31 - PubMed
-
- Frobell RB, Roos EM, Roos HP, Ranstam J, Lohmander LS. A randomized trial of treatment for acute anterior cruciate ligament tears. N Engl J Med. 2010July22;363(4):331-42 - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
