

Surgical strategy for isolated caudate lobectomy: experience with 16 cases
- PMID: 25100899
- PMCID: PMC4102013
- DOI: 10.1155/2014/983684
Surgical strategy for isolated caudate lobectomy: experience with 16 cases
Abstract
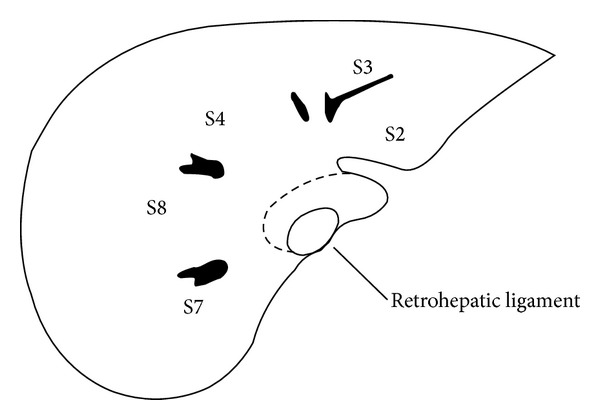
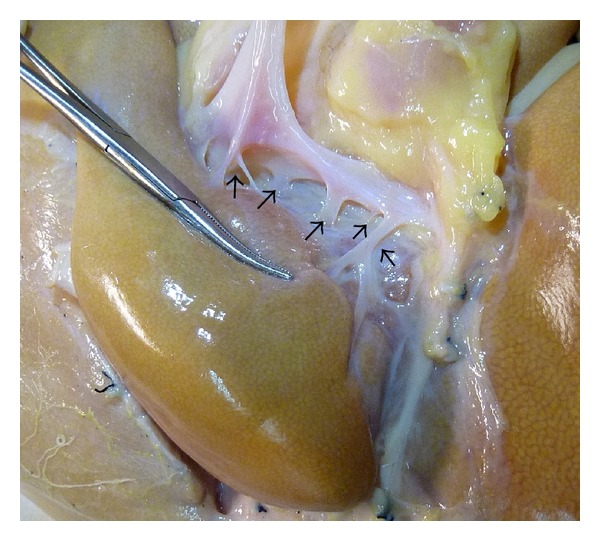
Introduction. Surgical resection is the most effective treatment for neoplasm in the caudate lobe. Isolated caudate lobectomy is still a challenge for hepatobiliary surgeons. No widely accepted surgical strategy for the procedure has been developed yet. Objective. To get a better understanding of isolated caudate lobectomy and to optimize the procedure. Materials and Methods. 16 cases of isolated caudate lobectomy were reviewed to summarize the surgical experience. Results. All the 16 cases of isolated caudate lobectomy were carried out successfully, among which left side approach was adopted in two cases (12.5%), right side approach in three cases (18.75%), and both sides approach in 11 cases (68.75%). No severe complications occurred. Conclusion. The majority of neoplasms confined to the caudate lobe can be resected safely by left and right side approach with proper anatomic surgical procedure, usually in the sequence of mobilization, outflow control, inflow control, and division of the hepatic parenchyma. Fully mobilizing the caudate lobe from the inferior vena cava (IVC) is of great importance. Division of the retrohepatic ligament and the venous ligament facilitated the procedure.
Figures
References
-
- Yamamoto T, Kubo S, Shuto T, et al. Surgical strategy for hepatocellular carcinoma originating in the caudate lobe. Surgery. 2004;135(6):595–603. - PubMed
-
- Kumon M. Anatomy of the caudate lobe with special reference to portal vein and bile duct. Acta Hepatologica Japonica. 1985;26(9):1193–1199.
-
- Couinaud C. The paracaval segments of the liver. Journal of Hepato-Biliary-Pancreatic Surgery. 1994;1(2):145–151.
-
- Hasegawa H, Cervens T-D, Yamasaki S, Kosuge T, Takayama T, Shimada K. Surgical strategy for hepatocellular carcinoma of the caudate lobe. Journal de Chirurgie. 1991;128(12):533–540. - PubMed
-
- Xu L-N, Huang Z-Q. Resection of hepatic caudate lobe hemangioma: experience with 11 patients. Hepatobiliary and Pancreatic Diseases International. 2010;9(5):487–491. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
