

Thalamic lesions: a radiological review
- PMID: 25100900
- PMCID: PMC4101959
- DOI: 10.1155/2014/154631
Thalamic lesions: a radiological review
Abstract
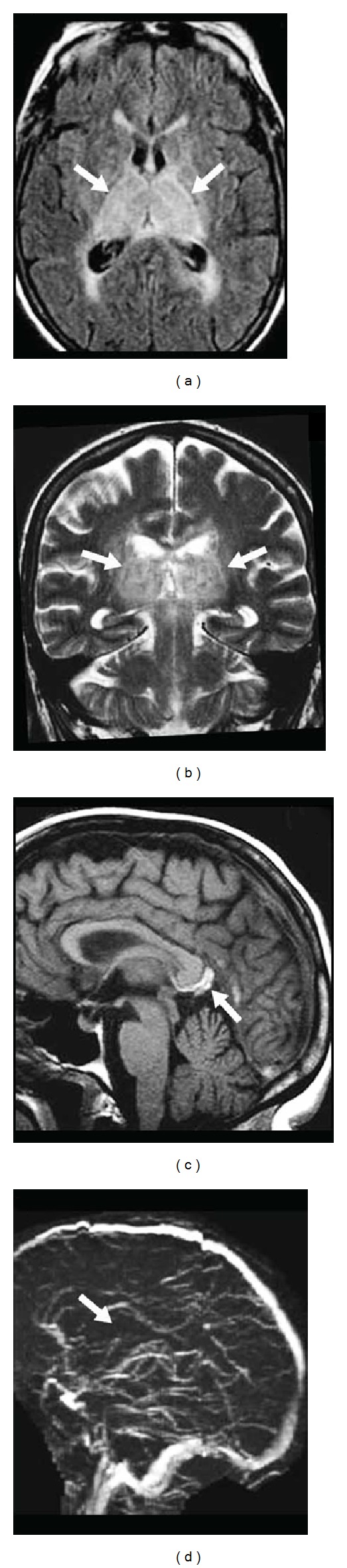
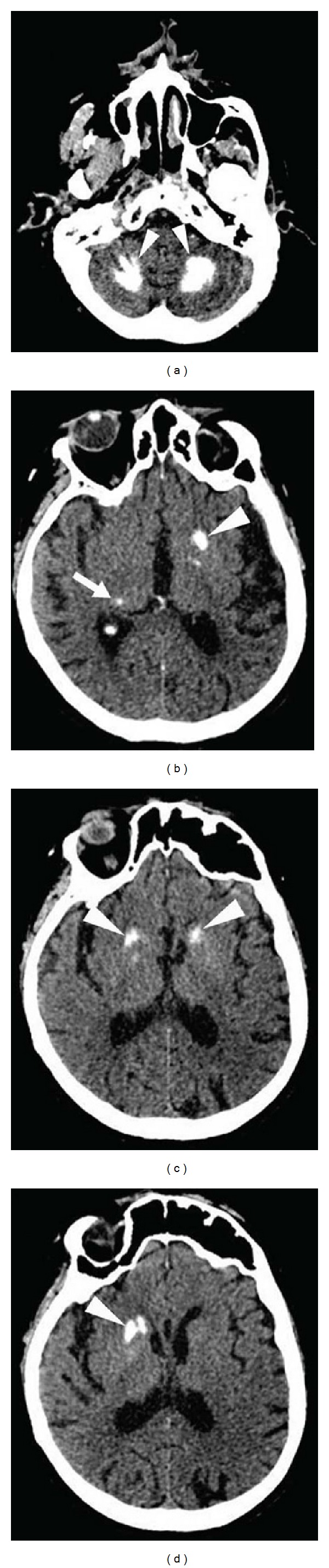
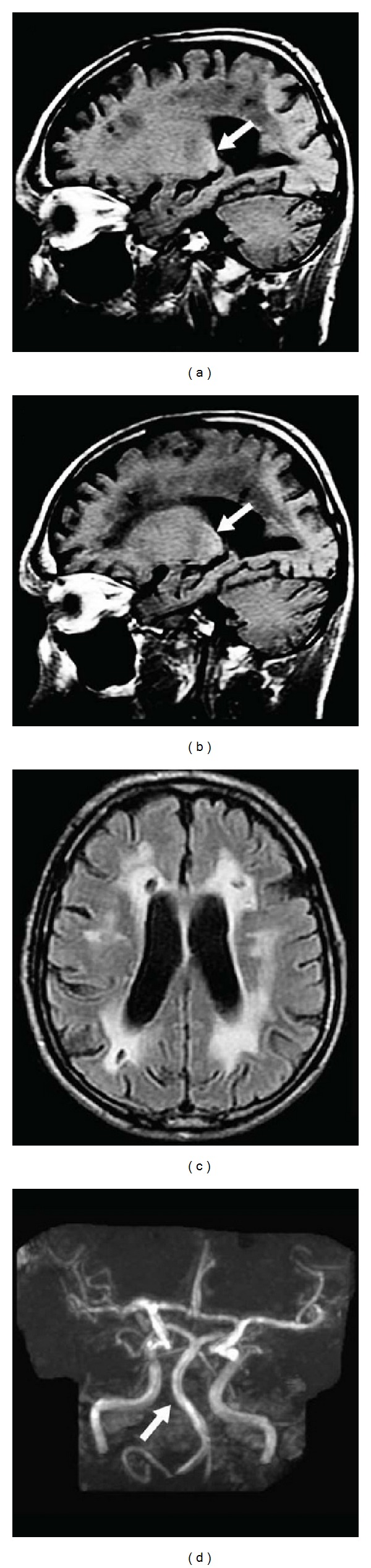
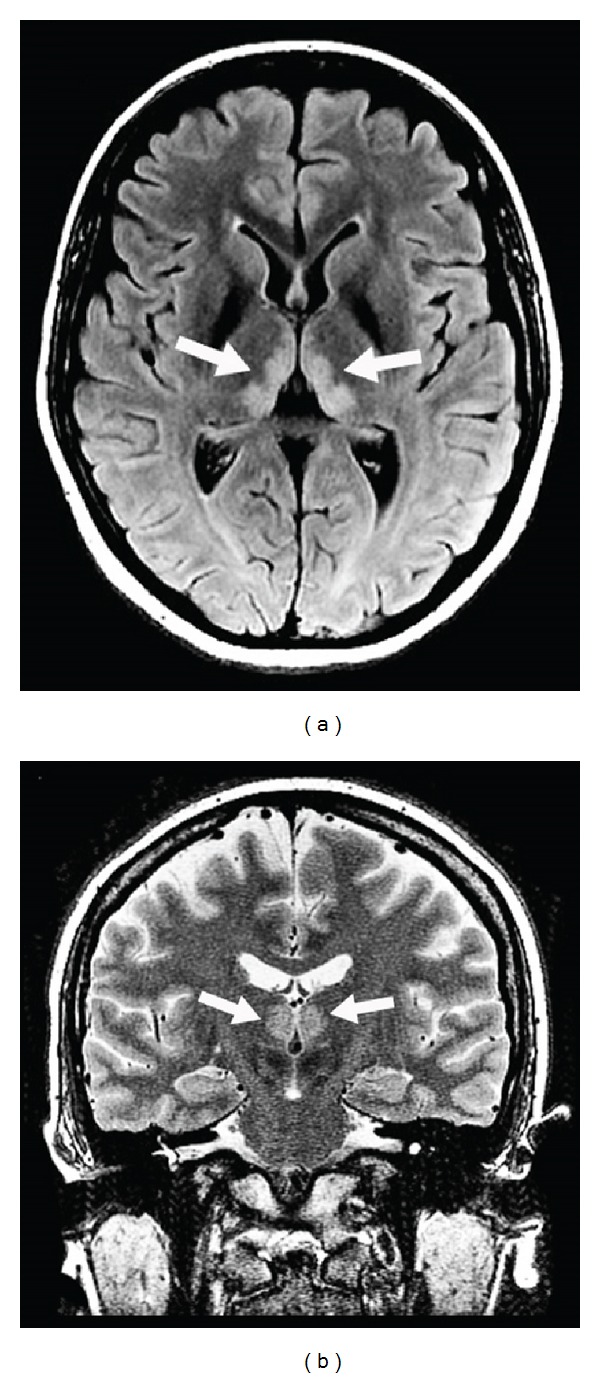
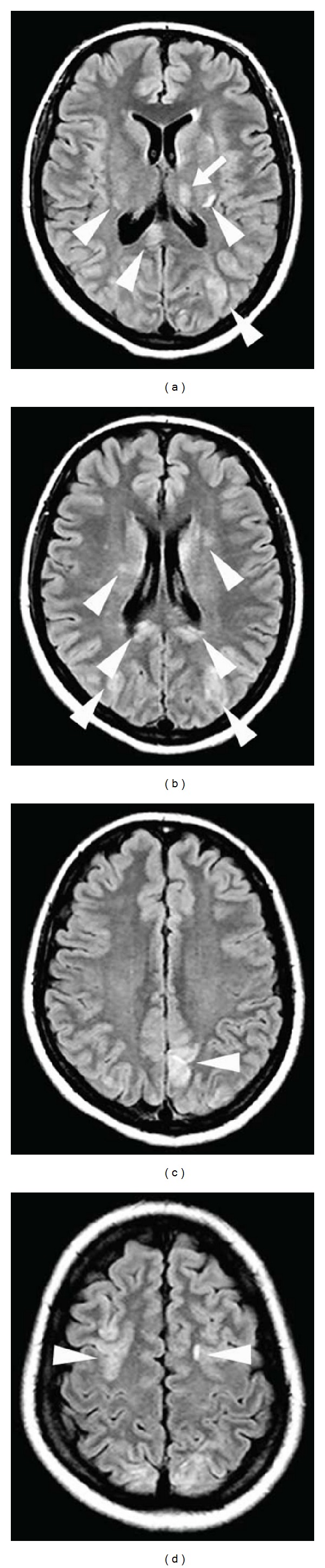
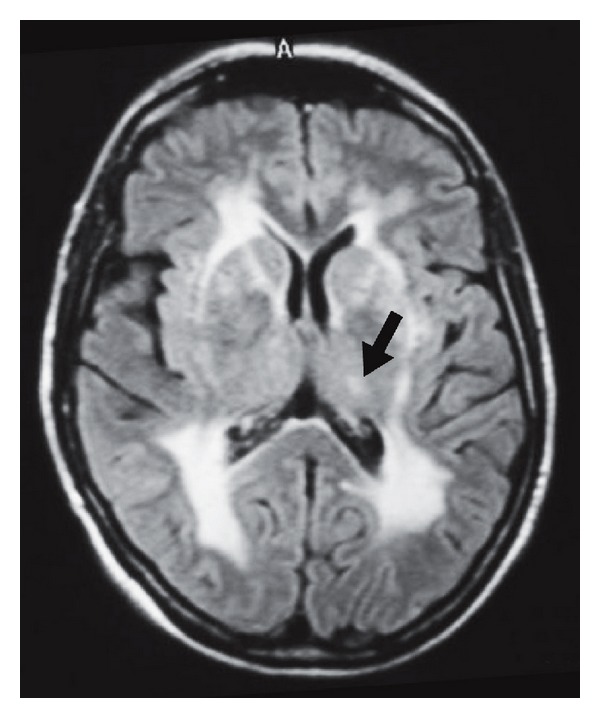
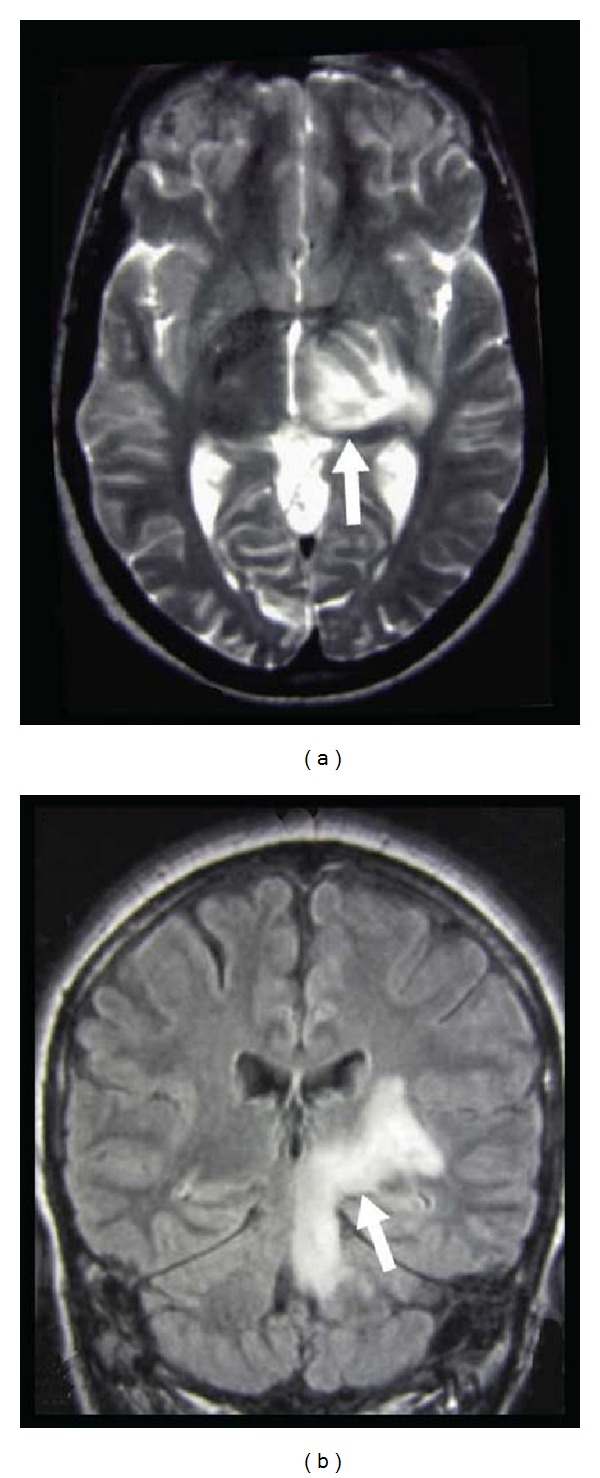
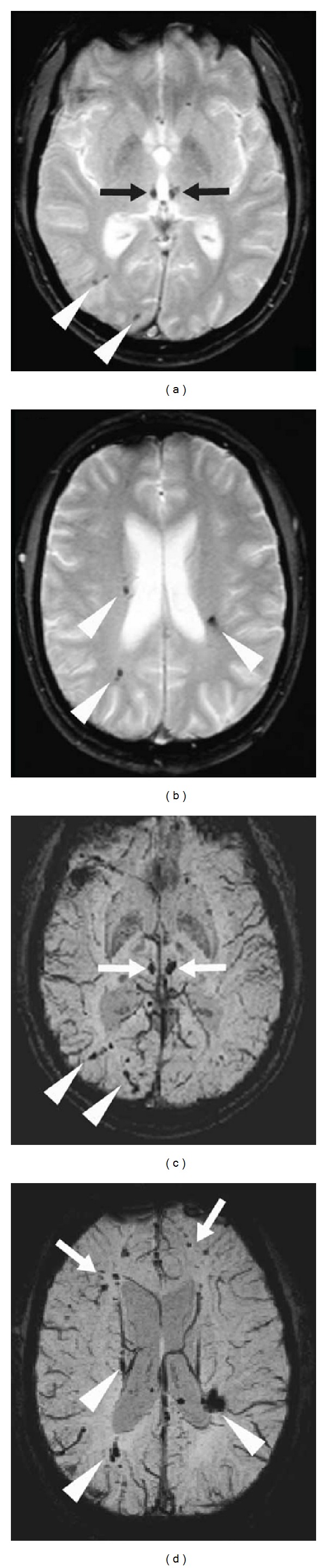
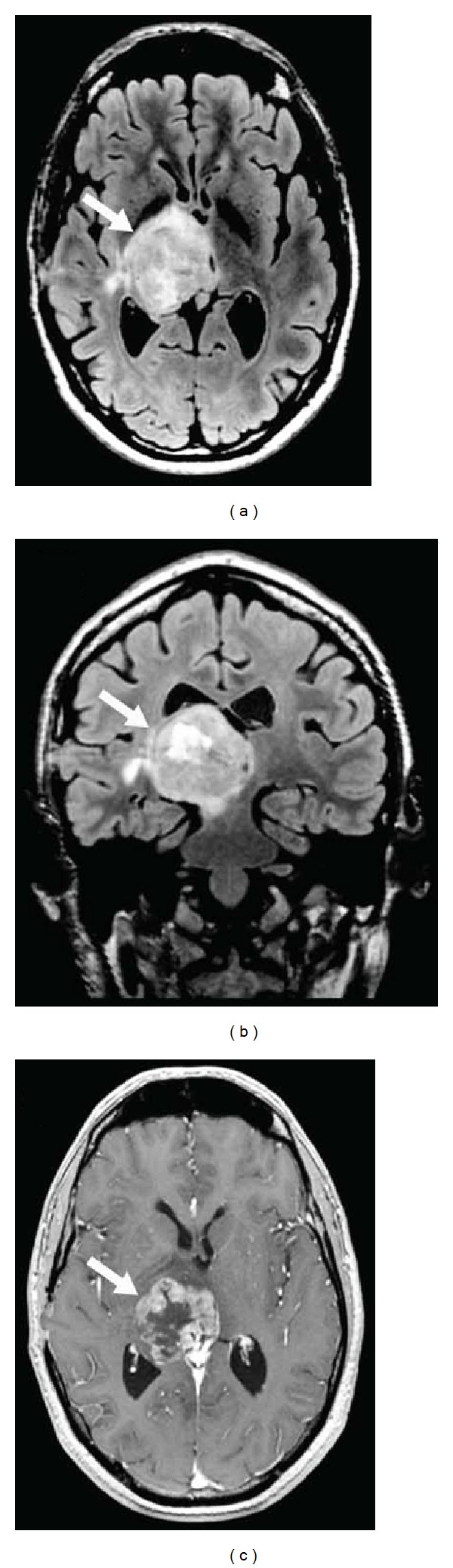
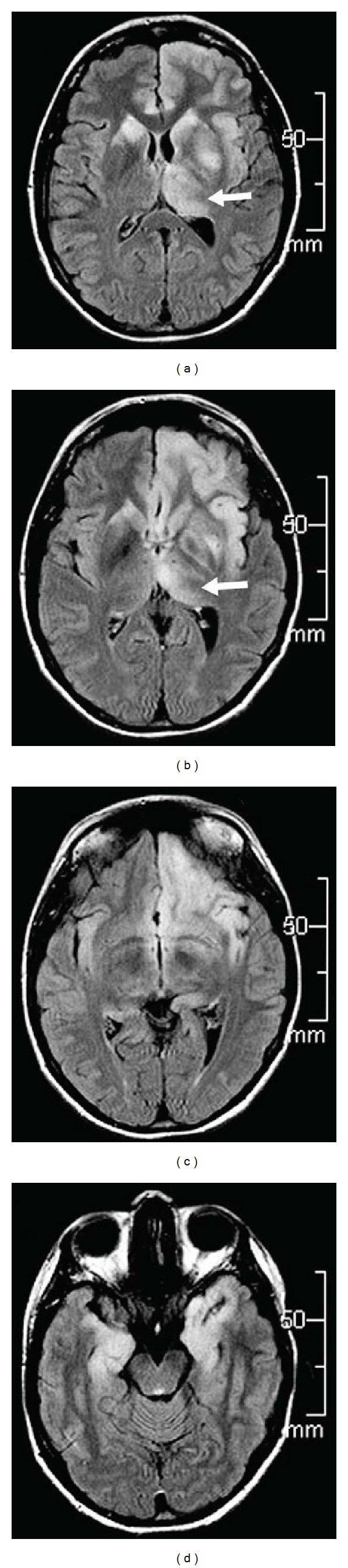
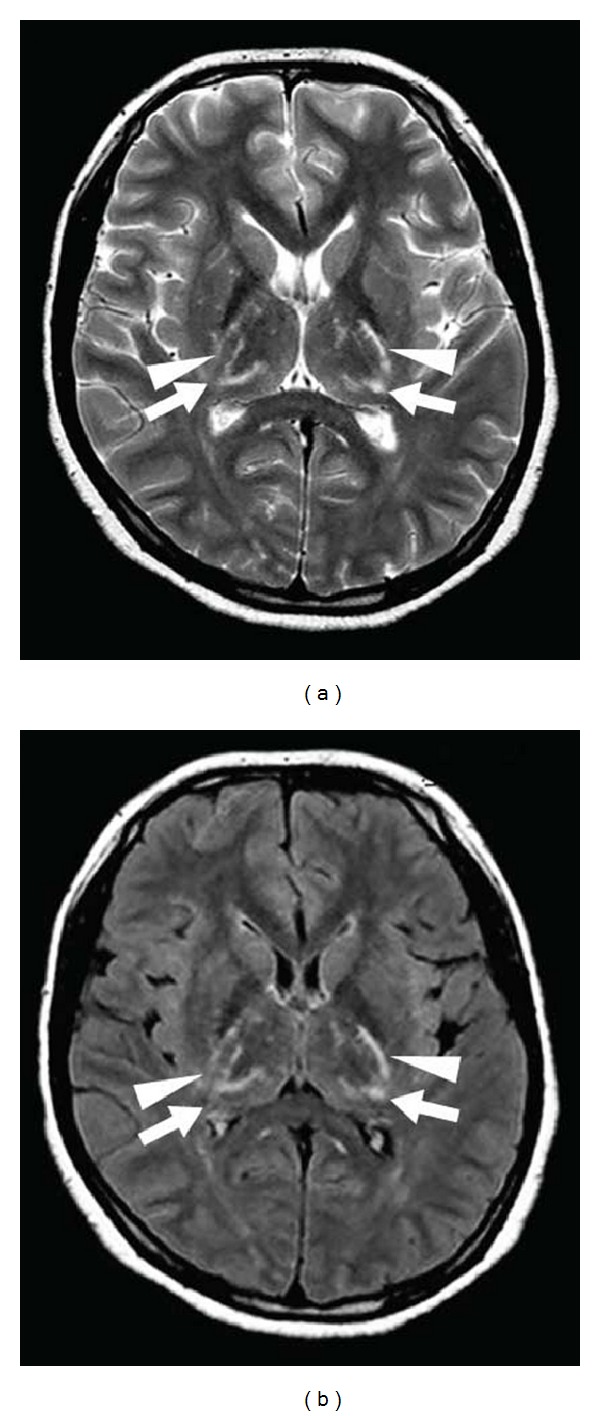
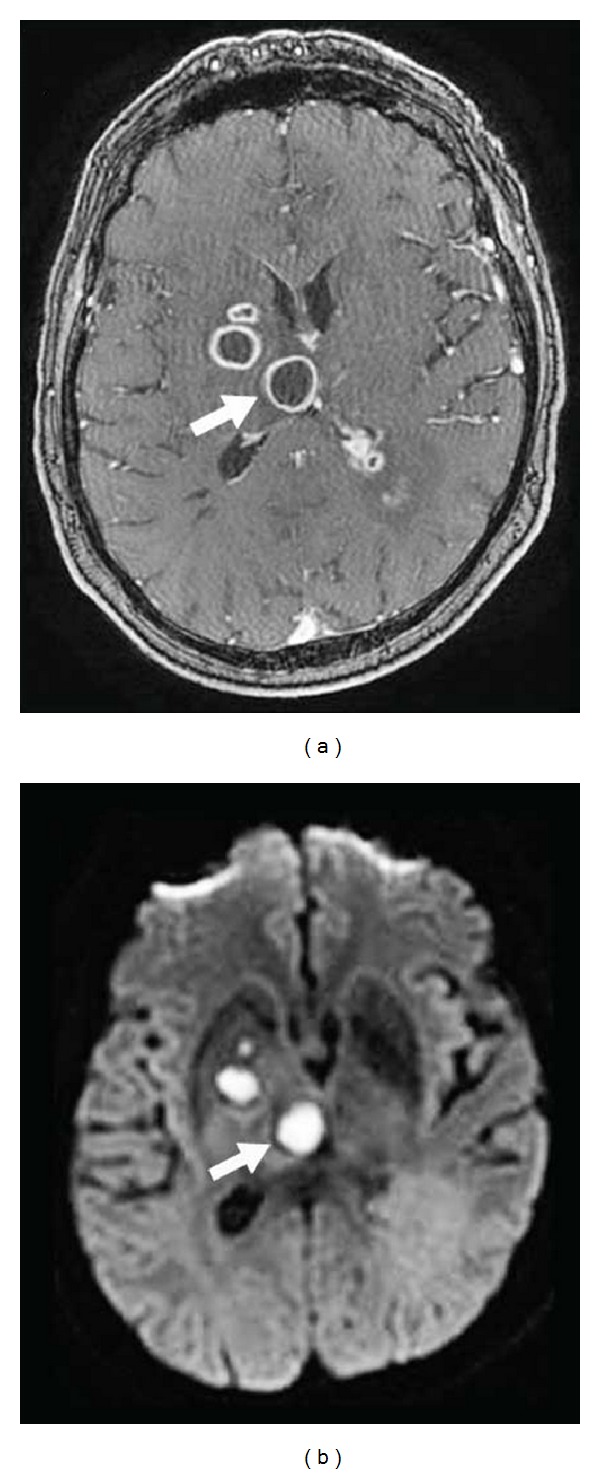
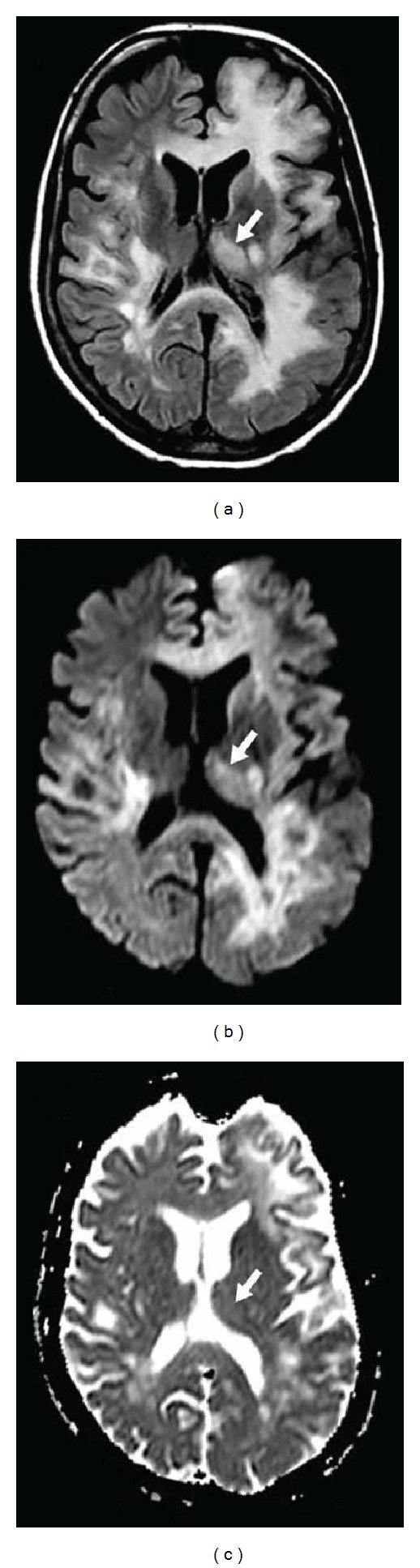
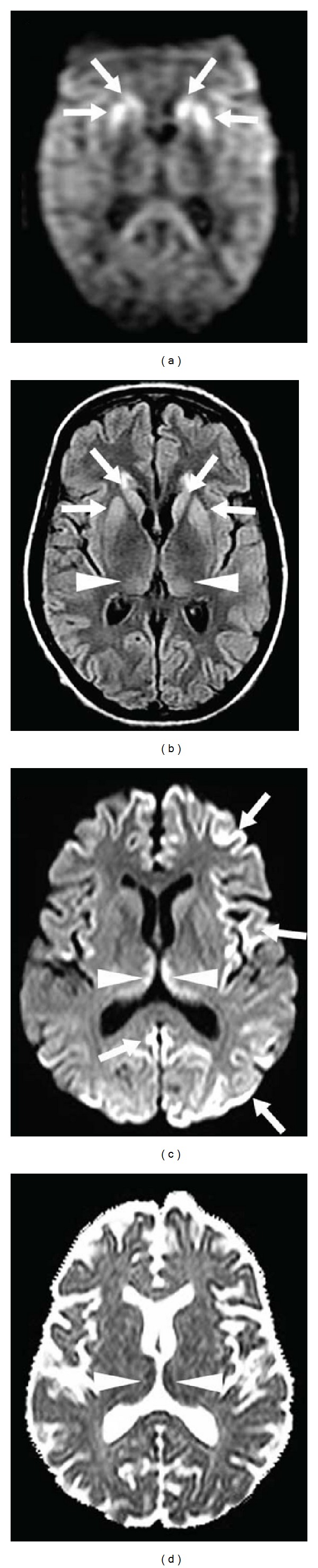
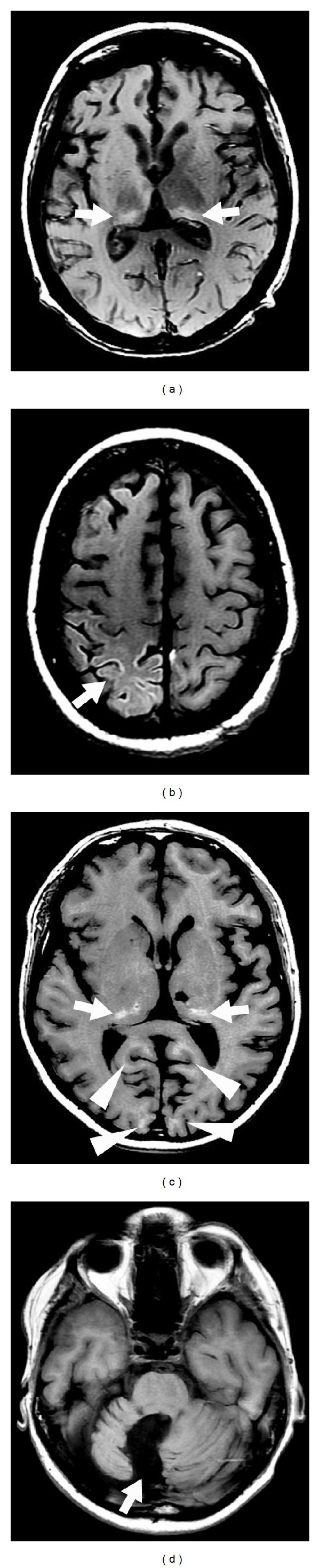
Background: Thalamic lesions are seen in a multitude of disorders including vascular diseases, metabolic disorders, inflammatory diseases, trauma, tumours, and infections. In some diseases, thalamic involvement is typical and sometimes isolated, while in other diseases thalamic lesions are observed only occasionally (often in the presence of other typical extrathalamic lesions).
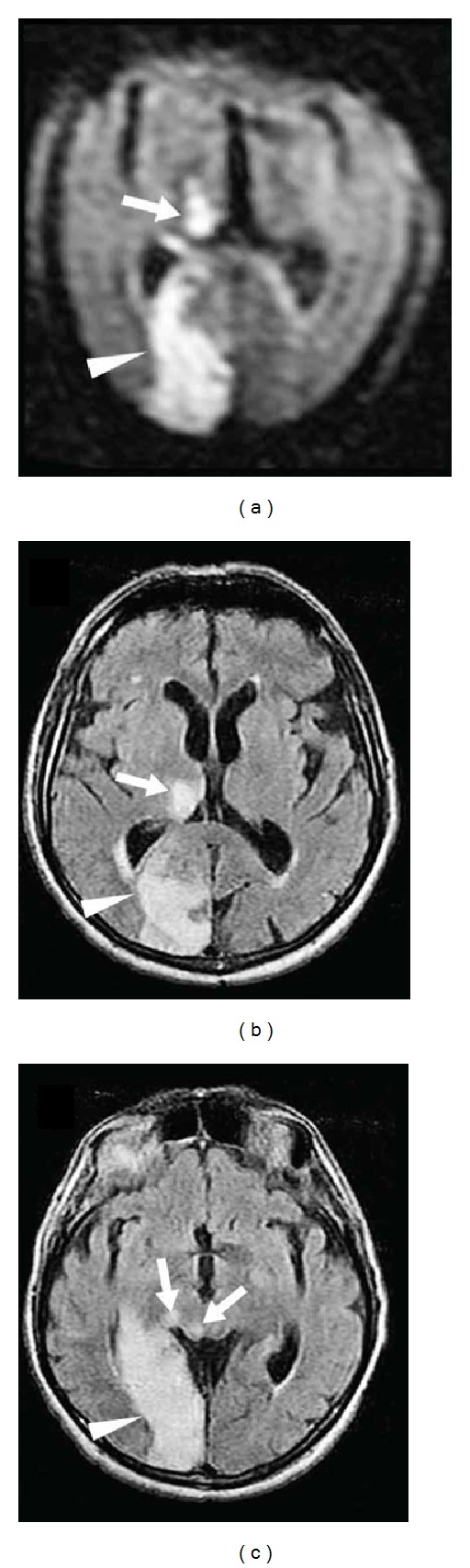
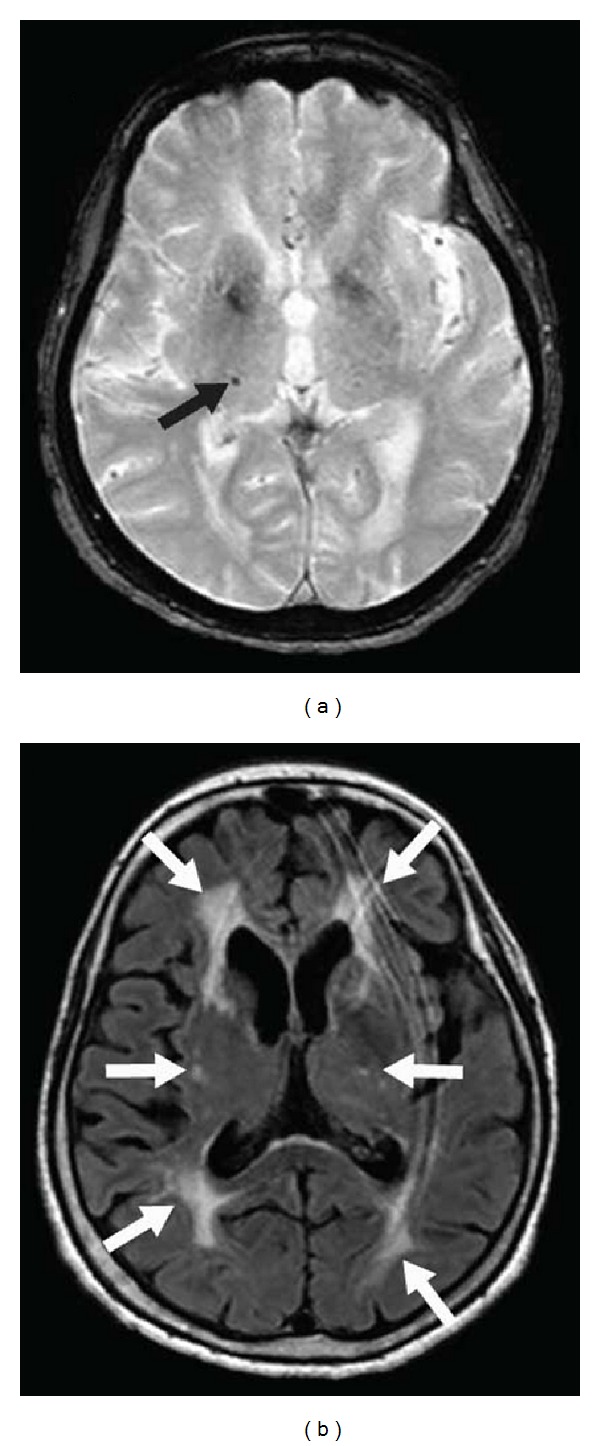
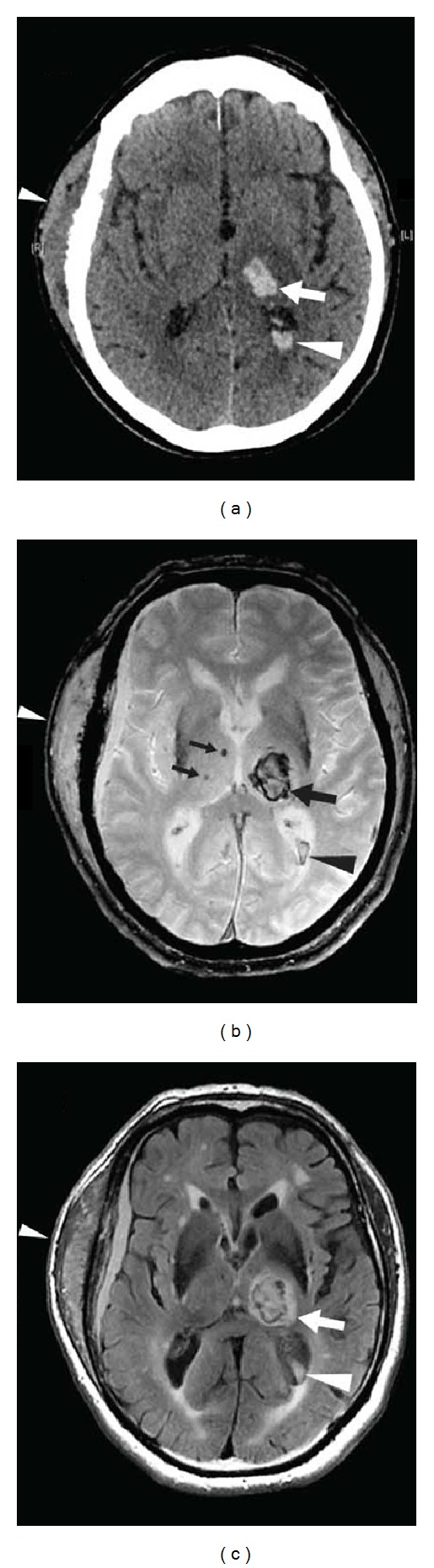
Summary: In this review, we will mainly discuss the MRI characteristics of thalamic lesions. Identification of the origin of the thalamic lesion depends on the exact localisation inside the thalamus, the presence of extrathalamic lesions, the signal changes on different MRI sequences, the evolution of the radiological abnormalities over time, the history and clinical state of the patient, and other radiological and nonradiological examinations.
Figures






Similar articles
-
An MRI review of acquired corpus callosum lesions.J Neurol Neurosurg Psychiatry. 2014 Sep;85(9):1041-8. doi: 10.1136/jnnp-2013-307072. Epub 2014 Feb 21. J Neurol Neurosurg Psychiatry. 2014. PMID: 24563521 Review.
-
Thalamic venous infarction as a cause of subacute dementia.Neurology. 2002 Jun 11;58(11):1689-91. doi: 10.1212/wnl.58.11.1689. Neurology. 2002. PMID: 12058103
-
[Differential diagnosis of bilateral thalamic lesions].Rofo. 2007 Mar;179(3):234-45. doi: 10.1055/s-2007-962857. Rofo. 2007. PMID: 17325992 German.
-
Brainstem lesions: MRI review of standard morphological sequences.Acta Neurol Belg. 2022 Jun;122(3):597-613. doi: 10.1007/s13760-022-01943-y. Epub 2022 Apr 15. Acta Neurol Belg. 2022. PMID: 35428930 Review.
-
Degeneration of paramedian nuclei in the thalamus induces Holmes tremor in a case of artery of Percheron infarction.Medicine (Baltimore). 2017 Nov;96(46):e8633. doi: 10.1097/MD.0000000000008633. Medicine (Baltimore). 2017. PMID: 29145285 Free PMC article.
Cited by
-
Bone-derived PDGF-BB drives brain vascular calcification in male mice.J Clin Invest. 2023 Dec 1;133(23):e168447. doi: 10.1172/JCI168447. J Clin Invest. 2023. PMID: 37815871 Free PMC article.
-
Incidental Thalamic Lesions Identified on Brain MRI in Pediatric and Young Adult Patients: Imaging Features and Natural History.AJNR Am J Neuroradiol. 2024 Feb 7;45(2):211-217. doi: 10.3174/ajnr.A8090. AJNR Am J Neuroradiol. 2024. PMID: 38238093 Free PMC article.
-
Bilateral Thalamic Stroke Arising From an Occlusion of the Artery of Percheron: Barriers to Diagnosis, Management, and Recovery.Cureus. 2021 Nov 21;13(11):e19783. doi: 10.7759/cureus.19783. eCollection 2021 Nov. Cureus. 2021. PMID: 34956778 Free PMC article.
-
Redefining the Pulvinar Sign in Fabry Disease.AJNR Am J Neuroradiol. 2017 Dec;38(12):2264-2269. doi: 10.3174/ajnr.A5420. Epub 2017 Oct 19. AJNR Am J Neuroradiol. 2017. PMID: 29051208 Free PMC article.
-
Bilateral thalamic changes in anti-NMDAR encephalitis presenting with hemichorea and dystonia and acute transient psychotic disorder.J Neuroimmunol. 2020 Oct 15;347:577329. doi: 10.1016/j.jneuroim.2020.577329. Epub 2020 Jul 22. J Neuroimmunol. 2020. PMID: 32745805 Free PMC article.
References
-
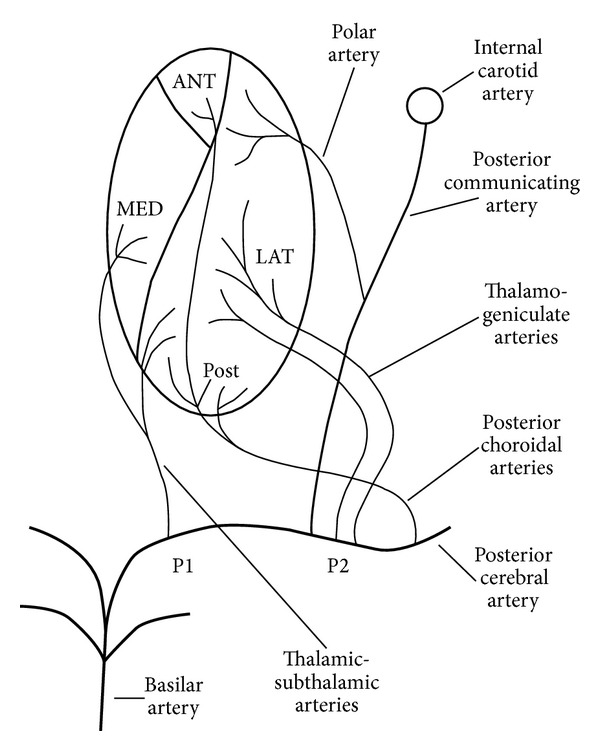
- Schmahmann JD. Vascular syndromes of the thalamus. Stroke. 2003;34:2264–2278. - PubMed
-
- Vinters HV. Cerebral amyloid angiopathy. A critical review. Stroke. 1987;18:311–324. - PubMed
-
- de Champfleur NM, Langlois C, Ankenbrandt WJ, et al. Magnetic resonance imaging evaluation of cerebral cavernous malformations with susceptibility-weighted imaging. Neurosurgery. 2011;68:641–647. - PubMed
-
- Reisin RC, Romero C, Marchesoni C, et al. Brain MRI findings in patients with Fabry disease. Journal of the Neurological Sciences. 2011;305(1):41–44. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
