

Computer-Assisted Planning and Patient-Specific Instruments for Bone Tumor Resection within the Pelvis: A Series of 11 Patients
- PMID: 25100921
- PMCID: PMC4101950
- DOI: 10.1155/2014/842709
Computer-Assisted Planning and Patient-Specific Instruments for Bone Tumor Resection within the Pelvis: A Series of 11 Patients
Abstract
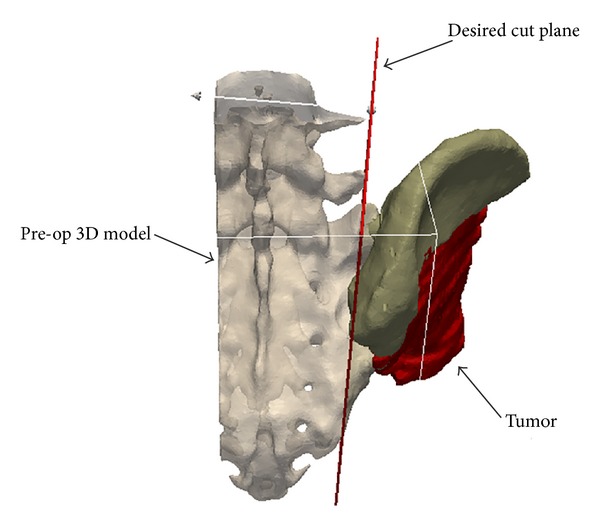
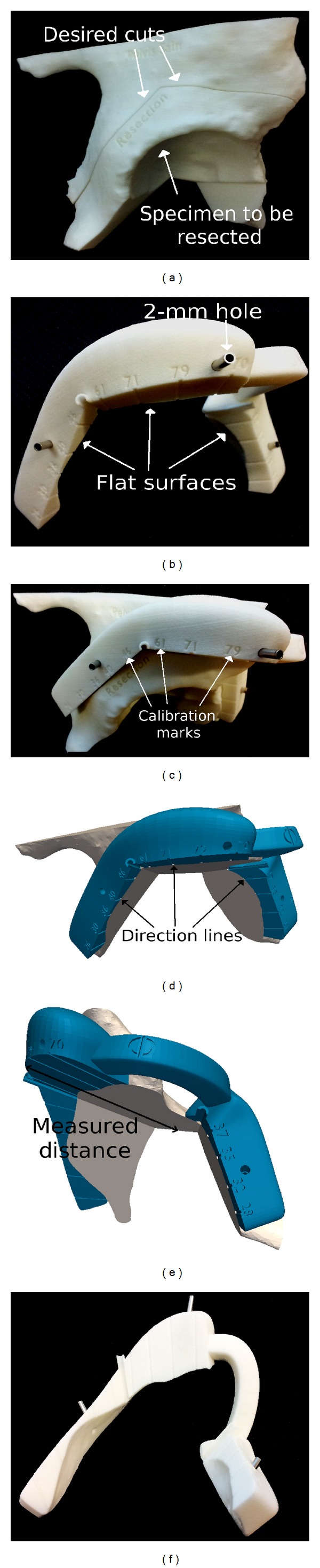
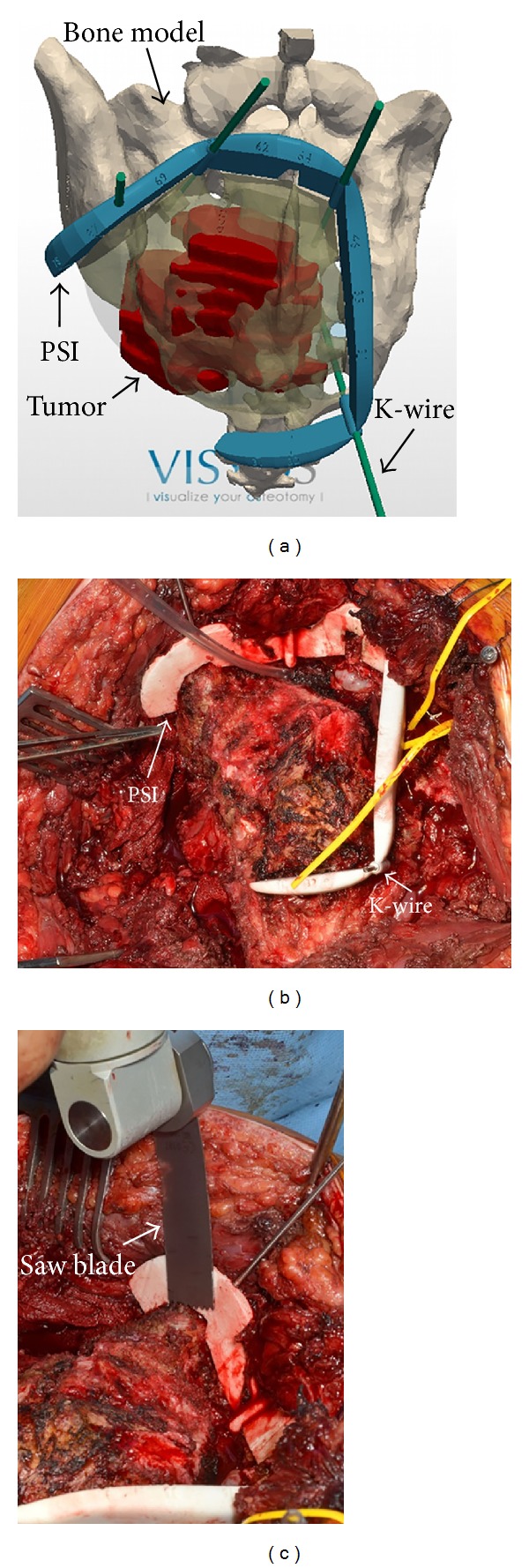
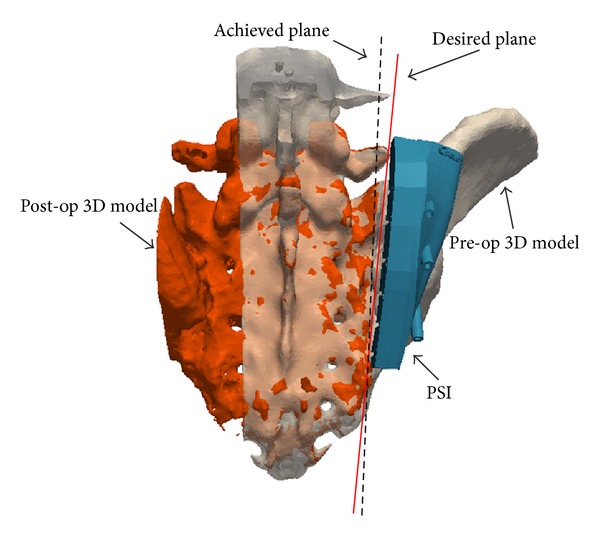
Pelvic bone tumor resection is challenging due to complex geometry, limited visibility, and restricted workspace. Accurate resection including a safe margin is required to decrease the risk of local recurrence. This clinical study reports 11 cases of pelvic bone tumor resected by using patient-specific instruments. Magnetic resonance imaging was used to delineate the tumor and computerized tomography to localize it in 3D. Resection planning consisted in desired cutting planes around the tumor including a safe margin. The instruments were designed to fit into unique position on the bony structure and to indicate the desired resection planes. Intraoperatively, instruments were positioned freehand by the surgeon and bone cutting was performed with an oscillating saw. Histopathological analysis of resected specimens showed tumor-free bone resection margins for all cases. Available postoperative computed tomography was registered to preoperative computed tomography to measure location accuracy (minimal distance between an achieved and desired cut planes) and errors on safe margin (minimal distance between the achieved cut planes and the tumor boundary). The location accuracy averaged 2.5 mm. Errors in safe margin averaged -0.8 mm. Instruments described in this study may improve bone tumor surgery within the pelvis by providing good cutting accuracy and clinically acceptable margins.
Figures
References
-
- Delloye C, Banse X, Brichard B, Docquier P, Cornu O. Pelvic reconstruction with a structural pelvic allograft after resection of a malignant bone tumor. Journal of Bone and Joint Surgery A. 2007;89(3):579–587. - PubMed
-
- Ozaki T, Flege S, Kevric M, et al. Osteosarcoma of the pelvis: experience of the Cooperative Osteosarcoma Study Group. Journal of Clinical Oncology. 2003;21(2):334–341. - PubMed
-
- Hoffmann C, Ahrens S, Dunst J, et al. Pelvic Ewing sarcoma: a retrospective analysis of 241 cases. Cancer. 1999;85(4):869–877. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
