

Pattern-recognition receptors and gastric cancer
- PMID: 25101079
- PMCID: PMC4105827
- DOI: 10.3389/fimmu.2014.00336
Pattern-recognition receptors and gastric cancer
Abstract
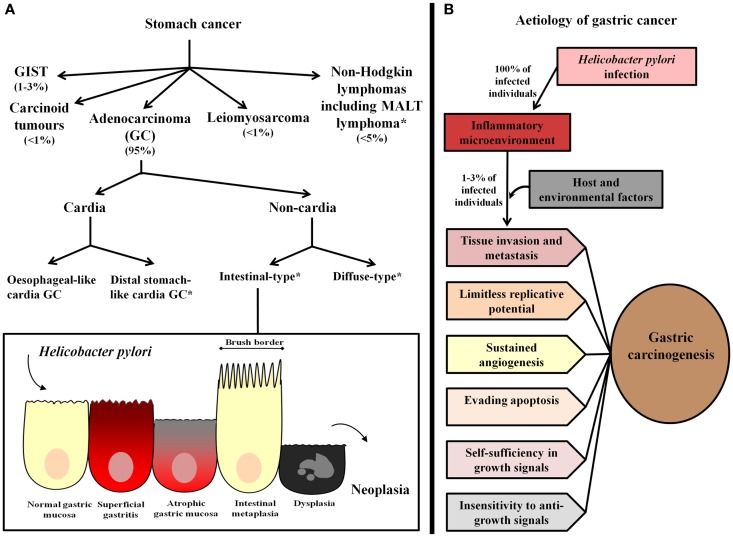
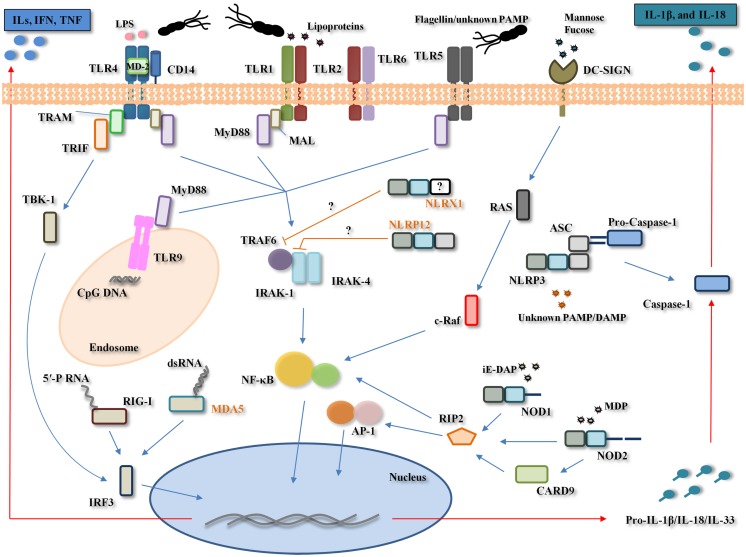
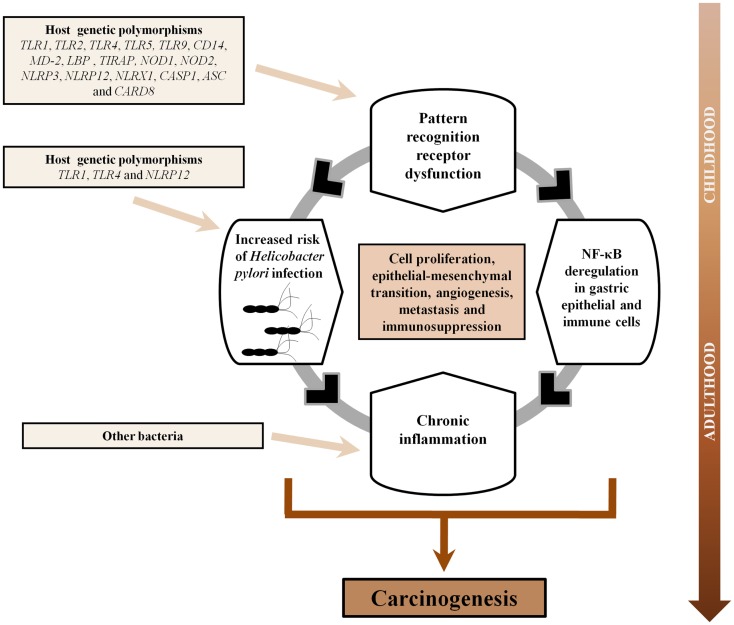
Chronic inflammation has been associated with an increased risk of several human malignancies, a classic example being gastric adenocarcinoma (GC). Development of GC is known to result from infection of the gastric mucosa by Helicobacter pylori, which initially induces acute inflammation and, in a subset of patients, progresses over time to chronic inflammation, gastric atrophy, intestinal metaplasia, dysplasia, and finally intestinal-type GC. Germ-line encoded receptors known as pattern-recognition receptors (PRRs) are critical for generating mature pro-inflammatory cytokines that are crucial for both Th1 and Th2 responses. Given that H. pylori is initially targeted by PRRs, it is conceivable that dysfunction within genes of this arm of the immune system could modulate the host response against H. pylori infection, and subsequently influence the emergence of GC. Current evidence suggests that Toll-like receptors (TLRs) (TLR2, TLR3, TLR4, TLR5, and TLR9), nucleotide-binding oligomerization domain (NOD)-like receptors (NLRs) (NOD1, NOD2, and NLRP3), a C-type lectin receptor (DC-SIGN), and retinoic acid-inducible gene (RIG)-I-like receptors (RIG-I and MDA-5), are involved in both the recognition of H. pylori and gastric carcinogenesis. In addition, polymorphisms in genes involved in the TLR (TLR1, TLR2, TLR4, TLR5, TLR9, and CD14) and NLR (NOD1, NOD2, NLRP3, NLRP12, NLRX1, CASP1, ASC, and CARD8) signaling pathways have been shown to modulate the risk of H. pylori infection, gastric precancerous lesions, and/or GC. Further, the modulation of PRRs has been suggested to suppress H. pylori-induced inflammation and enhance GC cell apoptosis, highlighting their potential relevance in GC therapeutics. In this review, we present current advances in our understanding of the role of the TLR and NLR signaling pathways in the pathogenesis of GC, address the involvement of other recently identified PRRs in GC, and discuss the potential implications of PRRs in GC immunotherapy.
Keywords: Helicobacter pylori; NOD-like receptors; Toll-like receptors; genetic polymorphism; inflammation; pattern-recognition receptors; stomach neoplasm; therapeutics.
Figures
Similar articles
-
The NOD-like receptor signalling pathway in Helicobacter pylori infection and related gastric cancer: a case-control study and gene expression analyses.PLoS One. 2014 Jun 5;9(6):e98899. doi: 10.1371/journal.pone.0098899. eCollection 2014. PLoS One. 2014. PMID: 24901306 Free PMC article.
-
The Relationship between Toll-like Receptors and Helicobacter pylori-Related Gastropathies: Still a Controversial Topic.J Immunol Res. 2019 Feb 4;2019:8197048. doi: 10.1155/2019/8197048. eCollection 2019. J Immunol Res. 2019. PMID: 30863783 Free PMC article. Review.
-
Pattern-recognition receptors in endometriosis: A narrative review.Front Immunol. 2023 Mar 23;14:1161606. doi: 10.3389/fimmu.2023.1161606. eCollection 2023. Front Immunol. 2023. PMID: 37033937 Free PMC article. Review.
-
Genetic polymorphisms in the Toll-like receptor signalling pathway in Helicobacter pylori infection and related gastric cancer.Hum Immunol. 2014 Aug;75(8):808-15. doi: 10.1016/j.humimm.2014.06.001. Epub 2014 Jun 11. Hum Immunol. 2014. PMID: 24929142
-
Toll-like receptors TLR4, TLR5 and TLR9 on gastric carcinoma cells: an implication for interaction with Helicobacter pylori.Int J Med Microbiol. 2005 Jun;295(3):179-85. doi: 10.1016/j.ijmm.2005.02.009. Int J Med Microbiol. 2005. PMID: 16044857
Cited by
-
Nucleotide-Binding Oligomerization Domain (NOD)-Like Receptor Subfamily C (NLRC) as a Prognostic Biomarker for Glioblastoma Multiforme Linked to Tumor Microenvironment: A Bioinformatics, Immunohistochemistry, and Machine Learning-Based Study.J Inflamm Res. 2023 Feb 10;16:523-537. doi: 10.2147/JIR.S397305. eCollection 2023. J Inflamm Res. 2023. PMID: 36798872 Free PMC article.
-
Roles of Plasmacytoid Dendritic Cells in Gastric Cancer.Front Oncol. 2022 Mar 3;12:818314. doi: 10.3389/fonc.2022.818314. eCollection 2022. Front Oncol. 2022. PMID: 35311157 Free PMC article. Review.
-
Toll-like receptor 2 and 4 polymorphisms associated with Helicobacter pylori susceptibility and gastric cancer.Turk J Gastroenterol. 2019 Jan;30(1):15-20. doi: 10.5152/tjg.2018.17461. Turk J Gastroenterol. 2019. PMID: 30301709 Free PMC article.
-
Innate Immunity Crosstalk with Helicobacter pylori: Pattern Recognition Receptors and Cellular Responses.Int J Mol Sci. 2022 Jul 8;23(14):7561. doi: 10.3390/ijms23147561. Int J Mol Sci. 2022. PMID: 35886908 Free PMC article. Review.
-
Oligometastatic Gastroesophageal Adenocarcinoma: Molecular Pathophysiology and Current Therapeutic Approach.Int J Mol Sci. 2020 Jan 31;21(3):951. doi: 10.3390/ijms21030951. Int J Mol Sci. 2020. PMID: 32023907 Free PMC article. Review.
References
-
- Ferlay J, Soerjomataram I, Ervik M, Dikshit R, Eser S, Mathers C, et al. GLOBOCAN 2012 v1.0, cancer incidence and mortality worldwide. IARC CancerBase No. 11 [Internet]. Lyon: International Agency for Research on Cancer; (2013).
-
- Hamilton SR, Aaltonen LA, editors. Tumours of the Digestive System. Lyon: IARC Press; (2000).
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous