

Cordectomy for intramedullary spinal cord glioblastoma with a 12-year survival
- PMID: 25101196
- PMCID: PMC4123255
- DOI: 10.4103/2152-7806.135305
Cordectomy for intramedullary spinal cord glioblastoma with a 12-year survival
Abstract
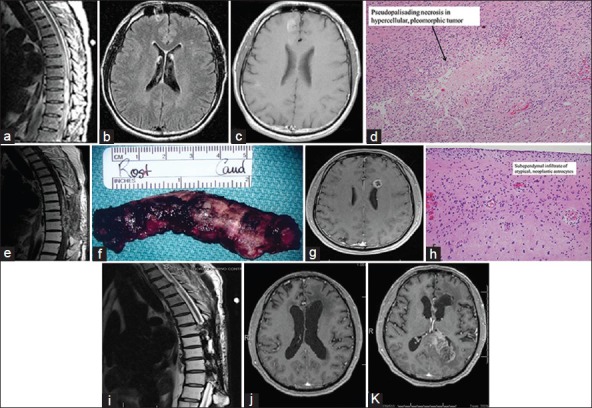
Background: Prognosis of patients with spinal cord glioblastoma is poor, with an average survival of 18 months. There are reports in the literature describing cordectomy as a treatment option for patients with spinal cord tumors.
Case description: This is a case report of a patient with spinal cord glioblastoma who, in addition to radiation and chemotherapy, was treated with cordectomy. Outcome of treatment resulted in 12-year survival.
Conclusion: Cordectomy in spinal cord glioblastoma can result in prolonged and meaningful survival.
Keywords: Cordectomy; ependymoma; neuro-oncology; spinal cord glioblastoma.
Figures
Similar articles
-
Multiple extraspinal recurrences of ependymoma 13 years after spinal cordectomy: case report.J Neurosurg Spine. 2018 Jul;29(1):92-96. doi: 10.3171/2017.12.SPINE17848. Epub 2018 Apr 27. J Neurosurg Spine. 2018. PMID: 29701571
-
Long-term cure of high-grade spinal cord glioma in a pediatric patient who underwent cordectomy.J Neurosurg Spine. 2015 Nov;23(5):635-641. doi: 10.3171/2015.7.SPINE15656. Epub 2015 Aug 7. J Neurosurg Spine. 2015. PMID: 26252785
-
Spinal cordectomy: A new hope for morbid spinal conditions.Clin Neurol Neurosurg. 2017 Jan;152:5-11. doi: 10.1016/j.clineuro.2016.11.003. Epub 2016 Nov 10. Clin Neurol Neurosurg. 2017. PMID: 27846400 Review.
-
Management of Patients with Primary Intramedullary Spinal Cord Glioblastoma.World Neurosurg. 2017 Feb;98:198-202. doi: 10.1016/j.wneu.2016.10.075. Epub 2016 Oct 21. World Neurosurg. 2017. PMID: 27777151
-
Primary Spinal Cord Small-Cell Glioblastoma: Case Report and Literature Review.World Neurosurg. 2018 Oct;118:69-70. doi: 10.1016/j.wneu.2018.07.007. Epub 2018 Jul 11. World Neurosurg. 2018. PMID: 30017760 Review.
Cited by
-
A Nomogram for Predicting Overall Survival of Patients With Primary Spinal Cord Glioblastoma.Neurospine. 2024 Jun;21(2):676-689. doi: 10.14245/ns.2448082.041. Epub 2024 Jun 30. Neurospine. 2024. PMID: 38955537 Free PMC article.
-
Evaluating the role of gross total resection in primary spinal cord glioblastoma: evidence from a multicenter cohort and meta-analysis.J Neurooncol. 2025 Jul 16. doi: 10.1007/s11060-025-05158-y. Online ahead of print. J Neurooncol. 2025. PMID: 40670812
-
Primary bulbo-medullary glioblastoma in a child: case report.Childs Nerv Syst. 2019 Dec;35(12):2417-2421. doi: 10.1007/s00381-019-04396-6. Epub 2019 Oct 30. Childs Nerv Syst. 2019. PMID: 31667535
-
Long-term survival after cordectomy in a case of spinal cord diffuse midline glioma, H3K27-altered: illustrative case.J Neurosurg Case Lessons. 2023 Dec 18;6(25):CASE23296. doi: 10.3171/CASE23296. Print 2023 Dec 18. J Neurosurg Case Lessons. 2023. PMID: 38109730 Free PMC article.
-
A Systematic Review on the Characteristics, Treatments and Outcomes of the Patients with Primary Spinal Glioblastomas or Gliosarcomas Reported in Literature until March 2015.PLoS One. 2016 Feb 9;11(2):e0148312. doi: 10.1371/journal.pone.0148312. eCollection 2016. PLoS One. 2016. PMID: 26859136 Free PMC article.
References
-
- Abel TJ, Chowdhary A, Thapa M, Rutledge JC, Geyer JR, Ojemann J, et al. Spinal cord pilocytic astrocytoma with leptomeningeal dissemination to the brain. Case report and review of the literature. J Neurosurg. 2006;105(6 Suppl):S508–14. - PubMed
-
- Alvisi C, Cerisoli M, Giulioni M. Intramedullary spinal gliomas: Long-term results of surgical treatments. Acta Neurochir (Wien) 1984;70:169–79. - PubMed
-
- Andrews AA, Enriques L, Renaudin J, Tomiyasu U. Spinal intramedullary glioblastoma with intracranial seeding. Report of a case. Arch Neurol. 1978;35:244–5. - PubMed
-
- Asano N, Kitamura K, Seo Y, Mukai K, Soga T, Hondo H, et al. Spinal cord glioblastoma multiforme with intracranial dissemination--case report. Neurol Med Chir (Tokyo) 1990;30:489–94. - PubMed
-
- Bell WO, Packer RJ, Seigel KR, Rorke LB, Sutton LN, Bruce DA, et al. Leptomeningeal spread of intramedullary spinal cord tumors. Report of three cases. J Neurosurg. 1988;69:295–300. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
