

Blake's pouch cyst
- PMID: 25101207
- PMCID: PMC4123264
- DOI: 10.4103/2152-7806.137533
Blake's pouch cyst
Abstract
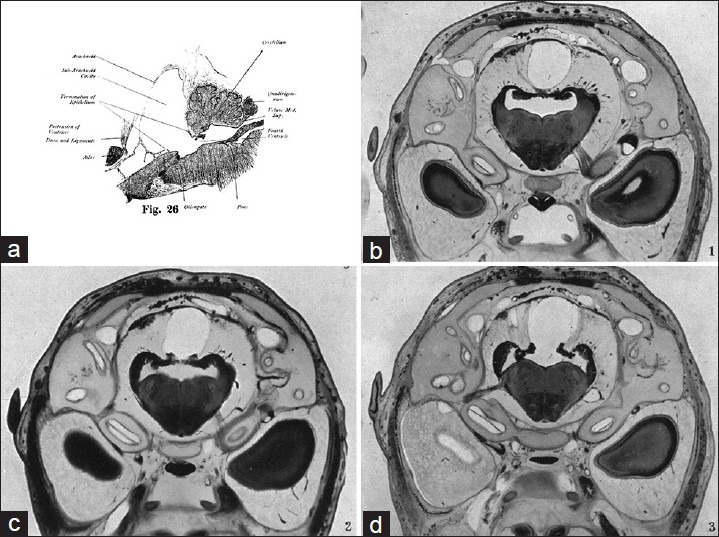
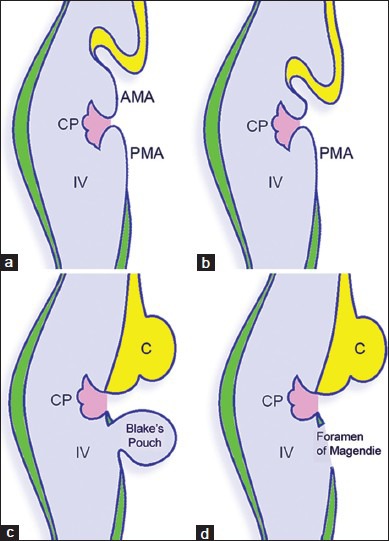
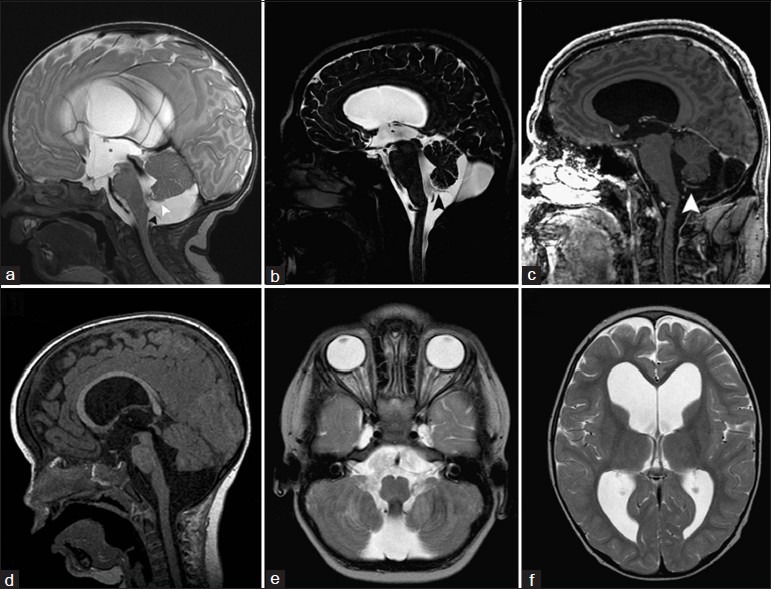
Background: In 1900, Joseph Blake described a transient posterior evagination of the tela choroidea of the fourth ventricle in the normal 130-day old human embryo. He was the first to recognize and fully elucidate on the real nature of the foramen of Magendie as an aperture, which develops within a saccular expansion of the embryonic fourth ventricular cavity. The persistence of this temporary fourth ventricular outpouching into the postnatal period and its significance either as separate entity or as an entity within the Dandy-Walker continuum has over the years been one of the most controversial topics in both neurosurgical and neuroradiological literature.
Methods: A search of the medical literature was conducted for publications addressing the historical, embryological, and neuororadiological features as well as the clinical presentation and management of persistent Blake's pouch.
Results: The literature on the various features of Blake's pouch cyst has limited areas of consensus between various authors.
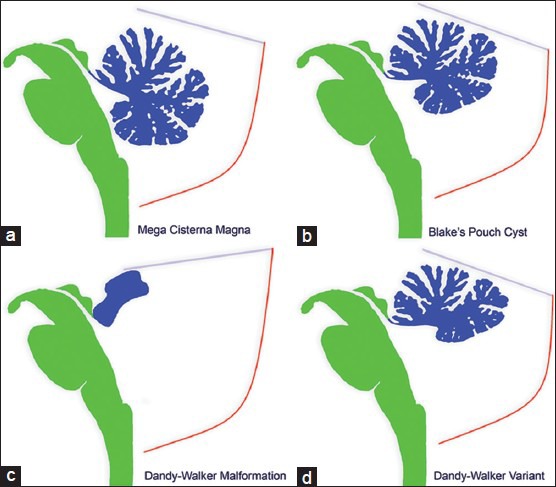
Conclusion: Blake's pouch cyst is a rare entity that is thought to belong to the Dandy-Walker continuum. It has a variable clinical presentation and when symptomatic can be treated with an endoscopic third ventriculostomy or shunting.
Keywords: Blake's pouch cyst; Dandy–Walker continuum; endoscopic; ventriculostomy.
Figures
References
-
- Arai H, Sato K. Posterior fossa cysts: Clinical, neuroradiological and surgical features. Childs Nerv Syst. 1991;7:156–64. - PubMed
-
- Barkovich AJ, Kjos BO, Norman D, Edwards MS. Revised classification of posterior fossa cysts and cystlike malformations based on the results of multiplanar MR imaging. AJR Am J Roentgenol. 1989;153:1289–300. - PubMed
-
- Barkovich AJ. Congenital malformations of the brain and skull. In: Barkovich AJ, editor. Pediatric Neuroimaging. 2nd ed. New York: Raven Press; 1994. pp. 177–275.
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
