

Modulation of HCV replication after combination antiretroviral therapy in HCV/HIV co-infected patients
- PMID: 25101888
- PMCID: PMC4326686
- DOI: 10.1126/scitranslmed.3008195
Modulation of HCV replication after combination antiretroviral therapy in HCV/HIV co-infected patients
Abstract
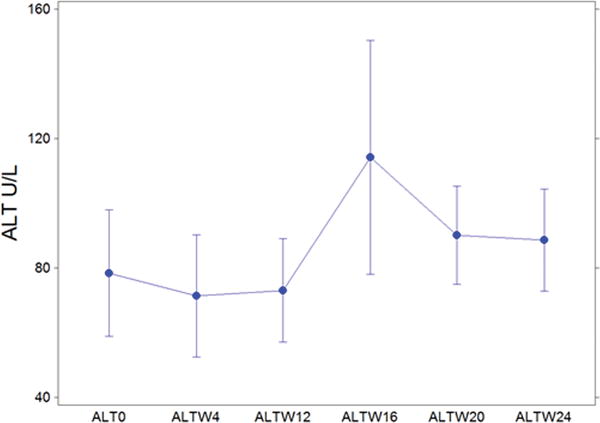
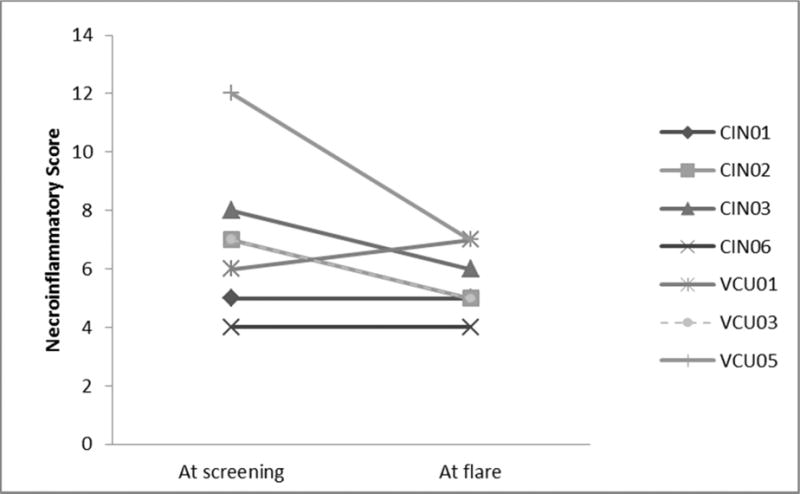
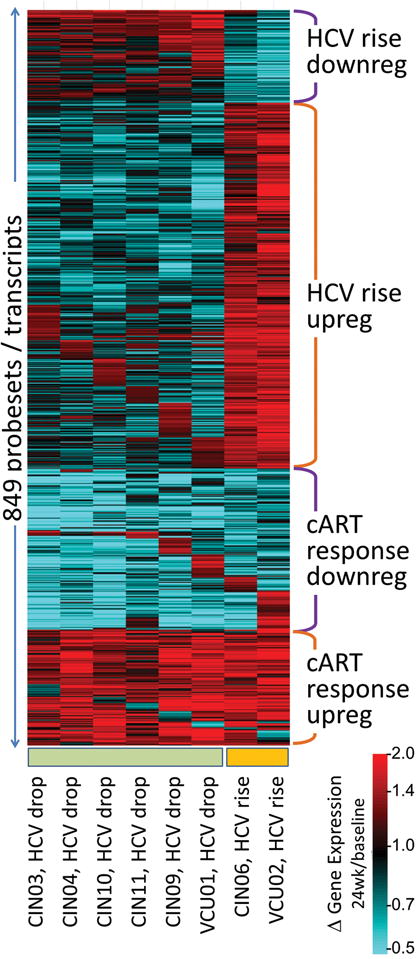
The hepatitis C virus (HCV) is an important contributor to morbidity and mortality in patients co-infected with HIV. Co-infection results in increased HCV replication and more rapid rates of liver disease progression. The effect of HIV combination antiretroviral therapy (cART) on HCV replication has not been studied in depth. To address this issue, we enrolled a small cohort of HCV/HIV co-infected patients into a cART initiation trial and used dynamic modeling combined with evaluation of immune responses and microarray profiles to determine how effective treatment of HIV affects HCV. Treatment with cART resulted in increased HCV replication and increased alanine aminotransferase (ALT) in a subset of patients. Subjects with evidence of hepatic injury (increased ALT) were more likely to have HCV-specific immune responses directed against HCV epitopes. Over time, HCV viral loads declined. Reproducible and biologically important gene expression changes occurred in co-infected patients who underwent successful cART. The effective suppression of HIV by cART initiated a cascade of early and late events in treated patients. Early events involving down-regulation of interferon-stimulated genes may have led to transiently increased viral replication and hepatic injury. At later time points, HCV viral load declined to levels comparable to those seen in the setting of HCV monoinfection. These findings support early antiretroviral therapy in those with HCV/HIV co-infection.
Copyright © 2014, American Association for the Advancement of Science.
Conflict of interest statement
Figures
Comment in
-
Infectious disease. HIV therapy good for HCV infection.Nat Rev Gastroenterol Hepatol. 2014 Sep;11(9):517. doi: 10.1038/nrgastro.2014.145. Epub 2014 Aug 5. Nat Rev Gastroenterol Hepatol. 2014. PMID: 25092043 No abstract available.
Similar articles
-
Impact of hepatitis C virus co-infection on HIV patients before and after highly active antiretroviral therapy: an immunological and clinical chemistry observation, Addis Ababa, Ethiopia.BMC Immunol. 2013 May 17;14:23. doi: 10.1186/1471-2172-14-23. BMC Immunol. 2013. PMID: 23679118 Free PMC article.
-
Transient liver injury associated with the early recovery of HCV-specific T-cell responses and HCV rebound in HIV-1/HCV coinfected patients undergoing highly active antiretroviral therapy.J Acquir Immune Defic Syndr. 2013 Feb 1;62(2):135-42. doi: 10.1097/QAI.0b013e3182752d20. J Acquir Immune Defic Syndr. 2013. PMID: 23075912
-
A switch to Raltegravir improves antiretroviral associated hepatotoxicity in individuals co-infected with HIV and hepatitis C.J Infect. 2014 Aug;69(2):190-3. doi: 10.1016/j.jinf.2014.04.005. Epub 2014 May 2. J Infect. 2014. PMID: 24793307
-
HIV and hepatitis C coinfection.J Gastroenterol Hepatol. 2008 Jul;23(7 Pt 1):1000-8. doi: 10.1111/j.1440-1746.2008.05489.x. J Gastroenterol Hepatol. 2008. PMID: 18707597 Review.
-
Efficacy of early treatment of acute hepatitis C infection with pegylated interferon and ribavirin in HIV-infected patients.AIDS. 2006 May 12;20(8):1157-61. doi: 10.1097/01.aids.0000226956.02719.fd. AIDS. 2006. PMID: 16691067 Review.
Cited by
-
CCR5 receptor antagonism inhibits hepatitis C virus (HCV) replication in vitro.PLoS One. 2019 Oct 29;14(10):e0224523. doi: 10.1371/journal.pone.0224523. eCollection 2019. PLoS One. 2019. PMID: 31661521 Free PMC article.
-
A changing paradigm: management and treatment of the HCV/HIV-co-infected patient.Hepatol Int. 2018 Nov;12(6):500-509. doi: 10.1007/s12072-018-9896-4. Epub 2018 Sep 20. Hepatol Int. 2018. PMID: 30238230 Free PMC article. Review.
-
Human immunodeficiency virus and liver disease: An update.Hepatology. 2015 Dec;62(6):1871-82. doi: 10.1002/hep.28150. Epub 2015 Oct 20. Hepatology. 2015. PMID: 26340591 Free PMC article.
-
A nonalcoholic fatty liver disease cirrhosis model in gerbil: the dynamic relationship between hepatic lipid metabolism and cirrhosis.Int J Clin Exp Pathol. 2018 Jan 1;11(1):146-157. eCollection 2018. Int J Clin Exp Pathol. 2018. PMID: 31938096 Free PMC article.
-
Hepatitis B and C infections in HIV-1 patients on combination antiretroviral therapy (cART) in Ghana: implications for immunologic recovery, clinical response to treatment, and hepatotoxicity.Heliyon. 2021 May 28;7(6):e07172. doi: 10.1016/j.heliyon.2021.e07172. eCollection 2021 Jun. Heliyon. 2021. PMID: 34141932 Free PMC article.
References
-
- Sherman K, Rouster S, Chung R, Rajicic N. Hepatitis C virus prevalence among patients infected with human immunodeficiency virus: a cross-sectional analysis of the US adult AIDS clinical trials groups. Clinical Infectious Diseases. 2002;34:831. - PubMed
-
- Sulkowski MS. Drug-induced liver injury associated with antiretroviral therapy that includes HIV-1 protease inhibitors. Clin Infect Dis. 2004 Mar 1;38(Suppl 2):S90. - PubMed
-
- Bonacini M, et al. Patients co-infected with human immunodeficiency virus and hepatitis C virus demonstrate higher levels of hepatic HCV RNA. J Viral Hepat. 1999;6:203. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
