

Does Braun enteroenterostomy reduce delayed gastric emptying after pancreaticoduodenectomy?
- PMID: 25101987
- PMCID: PMC4602449
- DOI: 10.1097/MD.0000000000000048
Does Braun enteroenterostomy reduce delayed gastric emptying after pancreaticoduodenectomy?
Abstract
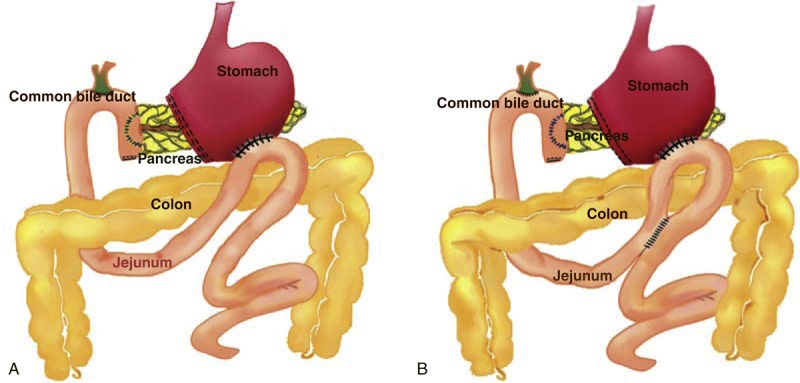
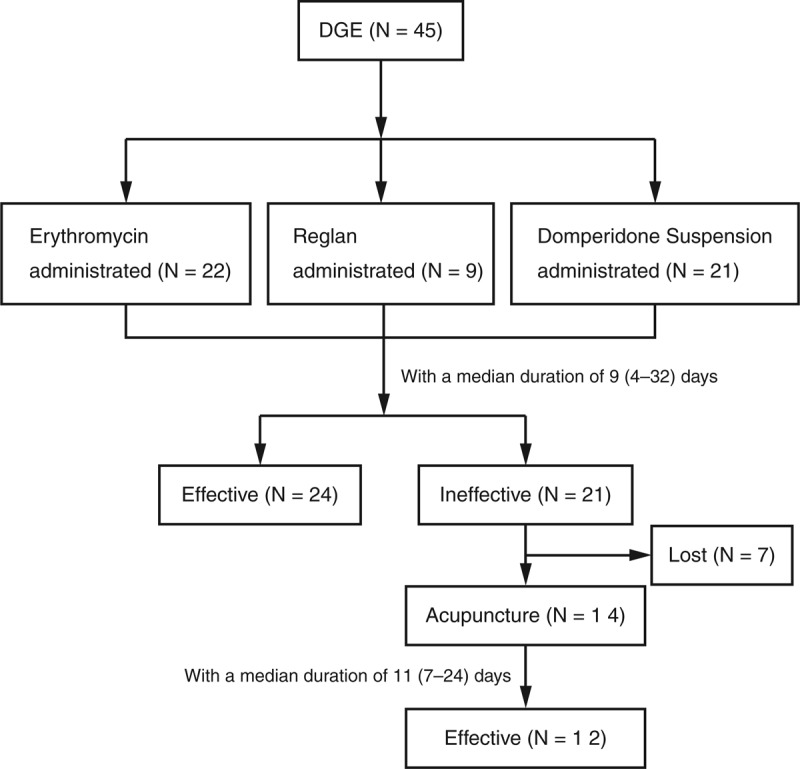
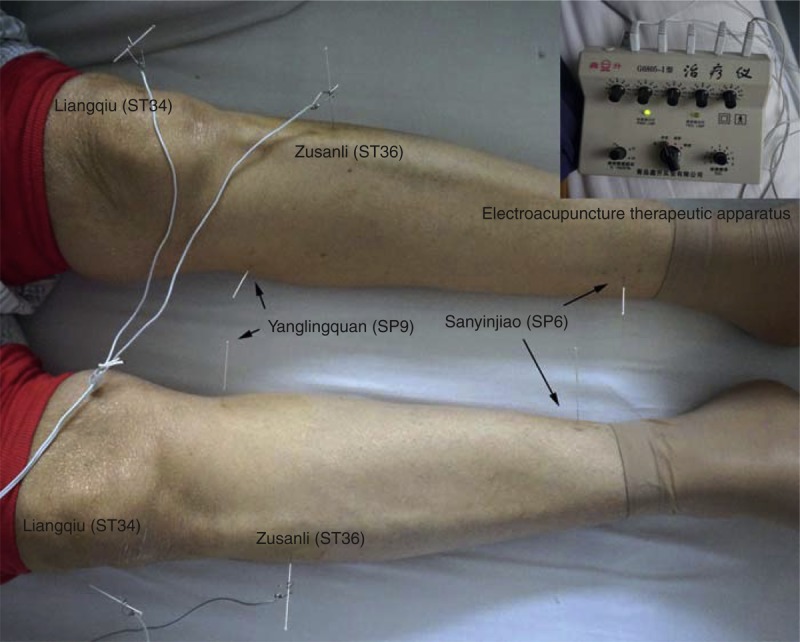
Whether an additional Braun enteroenterostomy is necessary in reducing delayed gastric emptying (DGE) after pancreaticoduodenectomy (PD) has not yet been well investigated. Herein, in this retrospective study, 395 consecutive cases of patients undergoing classic PD from 2009 to 2013 were reviewed. Patients with and without Braun enteroenterostomy were compared in preoperative baseline characteristics, surgical procedure, postoperative diagnosis, and morbidity including DGE. The DGE was defined and classified by the International Study Group of Pancreatic Surgery recommendation. The incidence of DGE was similar in patients with or without Braun enteroenterostomy following PD (37/347, 10.7% vs 8/48, 16.7%, P = 0.220). The patients in the 2 groups were not different in patient characteristics, lesions, surgical procedure, or postoperative complications, although patients without Braun enteroenterostomy more frequently presented postoperative vomiting than those with Braun enteroenterostomy (33.3% vs 15.3%, P = 0.002). Bile leakage, pancreatic fistula, and intraperitoneal abscess were risk factors for postoperative DGE (all P < 0.05). Prokinetic agents and acupuncture were effective in symptom relief of DGE in 24 out of 45 patients and 12 out of 14 patients, respectively.The additional Braun enteroenterostomy following classic PD was not associated with a decreased rate of DGE. Postoperative abdominal complications were strongly correlated with the onset of DGE. Prokinetic agents and acupuncture could be utilized in some patients with DGE.
Conflict of interest statement
The authors have no conflicts of interest to disclose.
Figures
Similar articles
-
Braun enteroenterostomy is associated with reduced delayed gastric emptying and early resumption of oral feeding following pancreaticoduodenectomy.J Surg Oncol. 2010 Apr 1;101(5):351-5. doi: 10.1002/jso.21490. J Surg Oncol. 2010. PMID: 20112274
-
Braun anastomosis lowers the incidence of delayed gastric emptying following pancreaticoduodenectomy: a meta-analysis.BMC Gastroenterol. 2018 Nov 26;18(1):176. doi: 10.1186/s12876-018-0909-5. BMC Gastroenterol. 2018. PMID: 30477442 Free PMC article.
-
Reduction in delayed gastric emptying following non-pylorus preserving pancreaticoduodenectomy by addition of a Braun enteroenterostomy.JOP. 2012 Sep 10;13(5):488-96. doi: 10.6092/1590-8577/800. JOP. 2012. PMID: 22964955 Clinical Trial.
-
Braun enteroenterostomy reduces delayed gastric emptying: A systematic review and meta-analysis.Int J Surg. 2015 Nov;23(Pt A):75-81. doi: 10.1016/j.ijsu.2015.09.038. Epub 2015 Sep 16. Int J Surg. 2015. PMID: 26384836
-
Braun enteroenterostomy during pancreaticoduodenectomy decreases postoperative delayed gastric emptying.Am J Surg. 2015 Jun;209(6):1036-42. doi: 10.1016/j.amjsurg.2014.06.035. Epub 2014 Oct 13. Am J Surg. 2015. PMID: 25457234
Cited by
-
Early enteral nutrition vs parenteral nutrition following pancreaticoduodenectomy: Experience from a single center.World J Gastroenterol. 2016 Apr 14;22(14):3821-8. doi: 10.3748/wjg.v22.i14.3821. World J Gastroenterol. 2016. PMID: 27076767 Free PMC article.
-
Does the Ileal Brake Contribute to Delayed Gastric Emptying After Pancreatoduodenectomy?Dig Dis Sci. 2017 Feb;62(2):319-335. doi: 10.1007/s10620-016-4402-0. Epub 2016 Dec 19. Dig Dis Sci. 2017. PMID: 27995402 Review.
-
PANCREATODUODENECTOMY: BRAZILIAN PRACTICE PATTERNS.Arq Bras Cir Dig. 2017 Jul-Sep;30(3):190-196. doi: 10.1590/0102-6720201700030007. Arq Bras Cir Dig. 2017. PMID: 29019560 Free PMC article.
-
Lengthened Efferent Limb in Braun Enteroenterostomy Reduces Delayed Gastric Emptying After Pancreaticoduodenectomy.World J Surg. 2023 May;47(5):1263-1270. doi: 10.1007/s00268-023-06925-6. Epub 2023 Jan 31. World J Surg. 2023. PMID: 36719447
-
Braun Enteroenterostomy Following Pancreaticoduodenectomy: A Systematic Review and Meta-Analysis.Medicine (Baltimore). 2015 Aug;94(32):e1254. doi: 10.1097/MD.0000000000001254. Medicine (Baltimore). 2015. PMID: 26266356 Free PMC article.
References
-
- Reed K, Vose PC, Jarstfer BS. Pancreatic 30 year review (1947 to 1977). Am J Surg. 1979;138:929–933. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
