

Modified tectonic keratoplasty with minimal corneal graft for corneal perforation in severe Stevens--Johnson syndrome: a case series study
- PMID: 25102918
- PMCID: PMC4129433
- DOI: 10.1186/1471-2415-14-97
Modified tectonic keratoplasty with minimal corneal graft for corneal perforation in severe Stevens--Johnson syndrome: a case series study
Abstract
Background: Corneal perforation in severe Stevens-Johnson syndrome (SJS) presenting great therapeutic difficulties, the imperative corneal transplantation always result in graft failure and repeated recurrence of perforation. The aim of this study was to evaluate the effectiveness of a modified small tectonic keratoplasty (MSTK) with minimal corneal graft in the management of refractory corneal perforation in severe SJS.
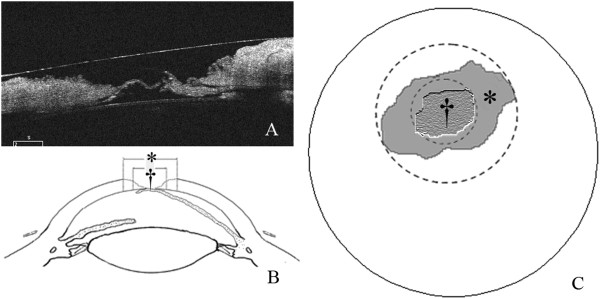
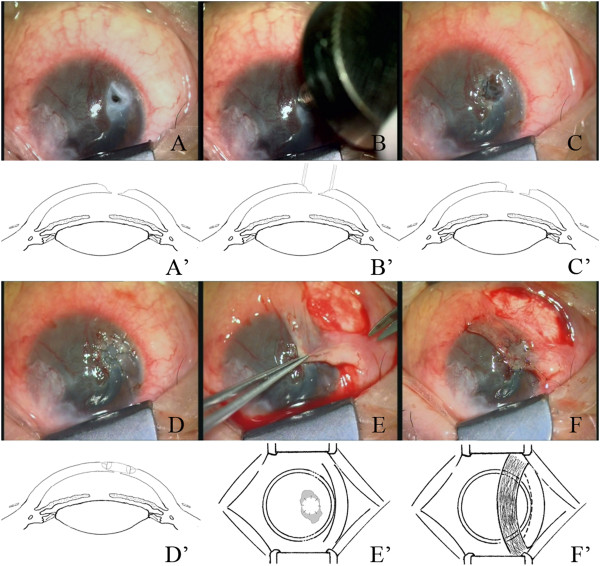
Methods: Refractory corneal perforations in ten patients (10 eyes) with severe SJS were mended with a minimal corneal patch graft, under the guidance of anterior chamber optical coherence tomography, combined with conjunctival flap covering. The outcome measures included healing of the corneal perforation, survival of the corneal graft and conjunctival flap, relevant complications, and improvement in visual acuity.
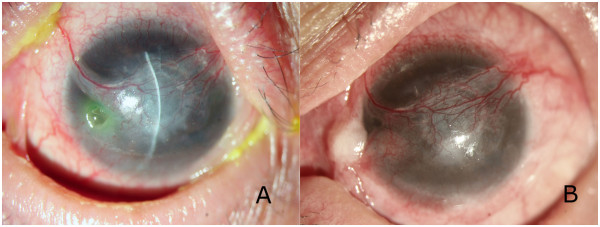
Results: Corneal perforation healed, and global integrity was achieved in all eyes. No immune rejection or graft melting was detected. Retraction of conjunctival flap occurred in one eye, which was treated with additional procedure. Visual acuity improved in six eyes (60%), unchanged in three eyes (30%) and declined in one eye (10%).
Conclusions: The MSTK combined with conjunctival flap covering seems to be effective for refractory corneal perforation in severe SJS.
Figures

Similar articles
-
DALK combined intralamellar tectonic patch graft: an alternative approach to treat frank corneal perforation.BMC Ophthalmol. 2023 Oct 27;23(1):436. doi: 10.1186/s12886-023-03179-7. BMC Ophthalmol. 2023. PMID: 37891524 Free PMC article.
-
[Boston Keratoprosthesis with temporal aponeurosis graft: A solution when there seems to be no more].J Fr Ophtalmol. 2018 Nov;41(9):830-835. doi: 10.1016/j.jfo.2018.01.010. Epub 2018 Oct 19. J Fr Ophtalmol. 2018. PMID: 30343989 French.
-
Penetrating keratoplasty in cicatrizing conjunctival diseases.Ophthalmology. 1995 Apr;102(4):576-85. doi: 10.1016/s0161-6420(95)30980-3. Ophthalmology. 1995. PMID: 7724175
-
Management of inflammatory corneal melt leading to central perforation in children: a retrospective study and review of literature.Eye (Lond). 2016 Apr;30(4):593-601. doi: 10.1038/eye.2015.278. Epub 2016 Jan 29. Eye (Lond). 2016. PMID: 26821761 Free PMC article. Review.
-
[Partial visual rehabilitation 5 and 6 years after a Gundersen total conjunctival flap procedure].Ophthalmologe. 2022 Feb;119(2):203-208. doi: 10.1007/s00347-021-01503-4. Epub 2021 Sep 28. Ophthalmologe. 2022. PMID: 34581853 Review. German.
Cited by
-
Autologous Tenon's patch graft: Techniques, clinical outcome, and complications in cases of immune corneal melt.Indian J Ophthalmol. 2025 Apr 1;73(4):563-566. doi: 10.4103/IJO.IJO_1890_24. Epub 2025 Mar 27. Indian J Ophthalmol. 2025. PMID: 40146143 Free PMC article.
-
Tectonic and Therapeutic Urgent Penetrating Keratoplasty Outcomes.Beyoglu Eye J. 2024 Jun 1;9(2):61-68. doi: 10.14744/bej.2024.69772. eCollection 2024. Beyoglu Eye J. 2024. PMID: 38854901 Free PMC article.
-
Active Pedicle Epithelial Flap Transposition Combined with Amniotic Membrane Transplantation for Treatment of Nonhealing Corneal Ulcers.J Ophthalmol. 2016;2016:5742346. doi: 10.1155/2016/5742346. Epub 2016 Oct 17. J Ophthalmol. 2016. PMID: 27830086 Free PMC article.
-
The outcomes of corneal sight rehabilitating surgery in Stevens-Johnson syndrome: case series.BMC Ophthalmol. 2024 May 6;24(1):205. doi: 10.1186/s12886-024-03461-2. BMC Ophthalmol. 2024. PMID: 38711013 Free PMC article.
-
Ocular sequelae of epidermal necrolysis: French national audit of practices, literature review and proposed management.Orphanet J Rare Dis. 2023 Mar 11;18(1):51. doi: 10.1186/s13023-023-02616-6. Orphanet J Rare Dis. 2023. PMID: 36906580 Free PMC article. Review.
References
-
- Lau B, Mutyala D, Dhaliwal D. A case report of doxycycline-induced Stevens-Johnson syndrome. Cornea. 2011;30:595–597. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
