

Emergency treatment of splenic injury in a novel mobile minimally invasive interventional shelter following disaster: a feasibility study
- PMID: 25103472
- PMCID: PMC4129467
- DOI: 10.1186/s13049-014-0044-4
Emergency treatment of splenic injury in a novel mobile minimally invasive interventional shelter following disaster: a feasibility study
Abstract
Background: There has been an increase in natural disasters in recent years, which leads to a great number of injuries and deaths. It still remains an unsolved problem to treat patients with vascular injury of solid organs effectively following natural disasters, but on-spot emergency interventional transcatheter arterial embolization (TAE) has been highly recommended to cure serious vascular injury of solid organs nowadays. Spleen is the most vulnerable abdominal organ, severe arterial hemorrhage of which can cause death if untreated timely. In this research, we aimed to study the possibility of performing emergency surgical intervention in mobile minimally invasive interventional shelter for splenic injury in the case of natural disasters.
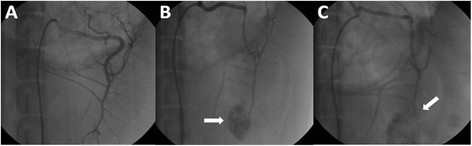
Methods: First, the mobile minimally invasive interventional shelter was unfolded in the field, and then disinfection and preoperative preparation were performed immediately. Eight large animal models of splenic injury were created, and angiograms were performed using a digital subtraction angiography machine in the mobile minimally invasive interventional shelter, and then the hemostatic embolizations of injured splenic artery were performed following the established convention of rapid intervention therapy. The operating time was recorded, and the survival condition and postoperative complications were observed for two weeks.
Results and discussion: The average time of unfolding the shelter, and performing disinfection and preoperative preparation was 33 ± 7 min. The number of colonies in the sterilized shelter body was 86 ± 13 cfu/m(3). The average TAE time was 31 ± 7 min. All the hemostatic embolizations of splenic injury were performed successfully in the mobile minimally invasive interventional shelter during the operation. A pseudoaneurysm was found in an animal model using angiography two weeks after the operation. The primary clinical success rate of embolization was 87.5%. The two-week survival rate in all animal models of splenic injury was 100%.
Conclusions: Our findings in the current study demonstrate that the mobile minimally invasive interventional shelter can be adapted to the field perfectly and complete emergency surgical intervention for splenic injury efficiently and safely. Therefore, on-spot emergency interventional TAE for vascular injury of solid organs (e.g. spleen) in mobile minimally invasive interventional shelter is available and effective.
Figures


Similar articles
-
A mobile minimally invasive interventional shelter: a new answer to on-spot emergency treatment of large arterial injuries?Scand J Trauma Resusc Emerg Med. 2015 Sep 4;23:63. doi: 10.1186/s13049-015-0144-9. Scand J Trauma Resusc Emerg Med. 2015. PMID: 26338214 Free PMC article.
-
Emergent transcatheter arterial embolization in hemodynamically unstable patients with blunt splenic injury.Acad Radiol. 2008 Feb;15(2):201-8. doi: 10.1016/j.acra.2007.09.010. Acad Radiol. 2008. PMID: 18206619
-
The usefulness of transcatheter arterial embolization for patients with blunt polytrauma showing transient response to fluid resuscitation.J Trauma. 2004 Aug;57(2):271-6; discussion 276-7. doi: 10.1097/01.ta.0000131198.79153.3c. J Trauma. 2004. PMID: 15345972
-
Nonoperative management of blunt splenic injury: what is new?Eur J Trauma Emerg Surg. 2015 Jun;41(3):219-28. doi: 10.1007/s00068-015-0520-1. Epub 2015 Apr 15. Eur J Trauma Emerg Surg. 2015. PMID: 26038038 Review.
-
Multidetector-row computed tomography imaging of splenic trauma.Semin Ultrasound CT MR. 2006 Oct;27(5):404-19. doi: 10.1053/j.sult.2006.06.007. Semin Ultrasound CT MR. 2006. PMID: 17048455 Review.
Cited by
-
A mobile minimally invasive interventional shelter: a new answer to on-spot emergency treatment of large arterial injuries?Scand J Trauma Resusc Emerg Med. 2015 Sep 4;23:63. doi: 10.1186/s13049-015-0144-9. Scand J Trauma Resusc Emerg Med. 2015. PMID: 26338214 Free PMC article.
-
Editorial: facts, figures and the future.Scand J Trauma Resusc Emerg Med. 2015 Jan 9;23:1. doi: 10.1186/s13049-014-0079-6. Scand J Trauma Resusc Emerg Med. 2015. PMID: 25583033 Free PMC article. No abstract available.
References
-
- Peitzman AB, Heil B, Rivera L, Federle MB, Harbrecht BG, Clancy KD, Croce M, Enderson BL, Morris JA, Shatz D. Blunt splenic injury in adults: multi-institutional study of the Eastern Association for the Surgery of Trauma. J Trauma Acute Care Surg. 2000;49:177–189. doi: 10.1097/00005373-200008000-00002. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
