

Pasireotide LAR maintains inhibition of GH and IGF-1 in patients with acromegaly for up to 25 months: results from the blinded extension phase of a randomized, double-blind, multicenter, Phase III study
- PMID: 25103549
- PMCID: PMC4424273
- DOI: 10.1007/s11102-014-0585-6
Pasireotide LAR maintains inhibition of GH and IGF-1 in patients with acromegaly for up to 25 months: results from the blinded extension phase of a randomized, double-blind, multicenter, Phase III study
Erratum in
-
Erratum to: Pasireotide LAR maintains inhibition of GH and IGF-1 in patients with acromegaly for up to 25 months: results from the blinded extension phase of a randomized, double-blind, multicenter, Phase III study.Pituitary. 2015 Jun;18(3):395-6. doi: 10.1007/s11102-014-0628-z. Pituitary. 2015. PMID: 25566750 Free PMC article. No abstract available.
Abstract
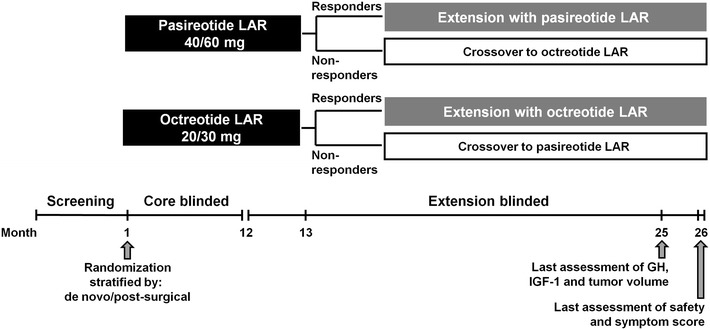
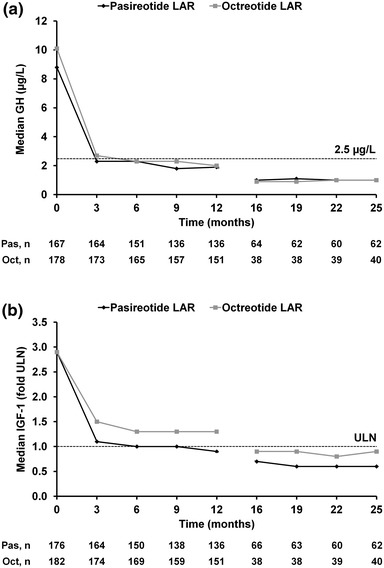
Purpose: A large, randomized, double-blind, Phase III core study demonstrated that pasireotide LAR was significantly superior to octreotide LAR at providing GH <2.5 μg/L and normalized IGF-1 after 12 months' treatment in patients with acromegaly. We report the efficacy and safety of pasireotide LAR and octreotide LAR after up to 26 months' treatment.
Methods: Patients with GH <2.5 μg/L and IGF-1 ≤1× ULN at month 12, or patients considered to be experiencing clinical benefit, were eligible to continue receiving their randomized therapy in the extension. Efficacy and safety in the pasireotide LAR and octreotide LAR groups were evaluated for up to 26 months.
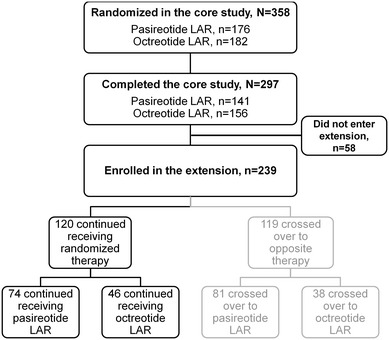
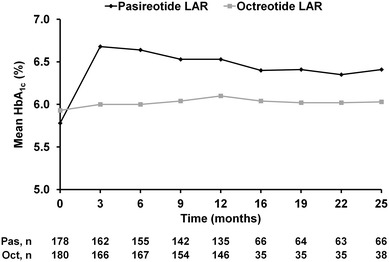
Results: Overall, 120 patients who completed the core study continued receiving pasireotide LAR (n = 74) or octreotide LAR (n = 46) in the extension. At month 25, biochemical control (GH <2.5 μg/L and normal IGF-1) was achieved by 48.6% (36/74) and 45.7% (21/46) of patients in the pasireotide LAR and octreotide LAR arms [60.8% (45/74) and 52.2% (24/46) when including patients with IGF-1 < LLN], respectively. In total, 74.7% of pasireotide LAR and 71.6% of octreotide LAR patients had tumor volume decrease ≥20% from baseline to month 26. Most AEs were mild or moderate. Hyperglycemia-related AEs were seen in 62.9 and 25.0% of pasireotide LAR and octreotide LAR patients, respectively. No new safety signals were observed in the extension compared with the core study.
Conclusions: GH and IGF-1 suppression is maintained for up to 25 months during pasireotide LAR treatment. The safety profile of pasireotide LAR is typical of a somatostatin analogue, except for the frequency and degree of hyperglycemia.
Trial registration: ClinicalTrials.gov NCT00600886.
Figures
References
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
