

Extent of coronary and myocardial disease and benefit from surgical revascularization in ischemic LV dysfunction [Corrected]
- PMID: 25104523
- PMCID: PMC4129547
- DOI: 10.1016/j.jacc.2014.04.064
Extent of coronary and myocardial disease and benefit from surgical revascularization in ischemic LV dysfunction [Corrected]
Erratum in
- J Am Coll Cardiol. 2014 Oct 7;64(14):1539
Abstract
Background: Patients with ischemic left ventricular dysfunction have higher operative risk with coronary artery bypass graft surgery (CABG). However, those whose early risk is surpassed by subsequent survival benefit have not been identified.
Objectives: This study sought to examine the impact of anatomic variables associated with poor prognosis on the effect of CABG in ischemic cardiomyopathy.
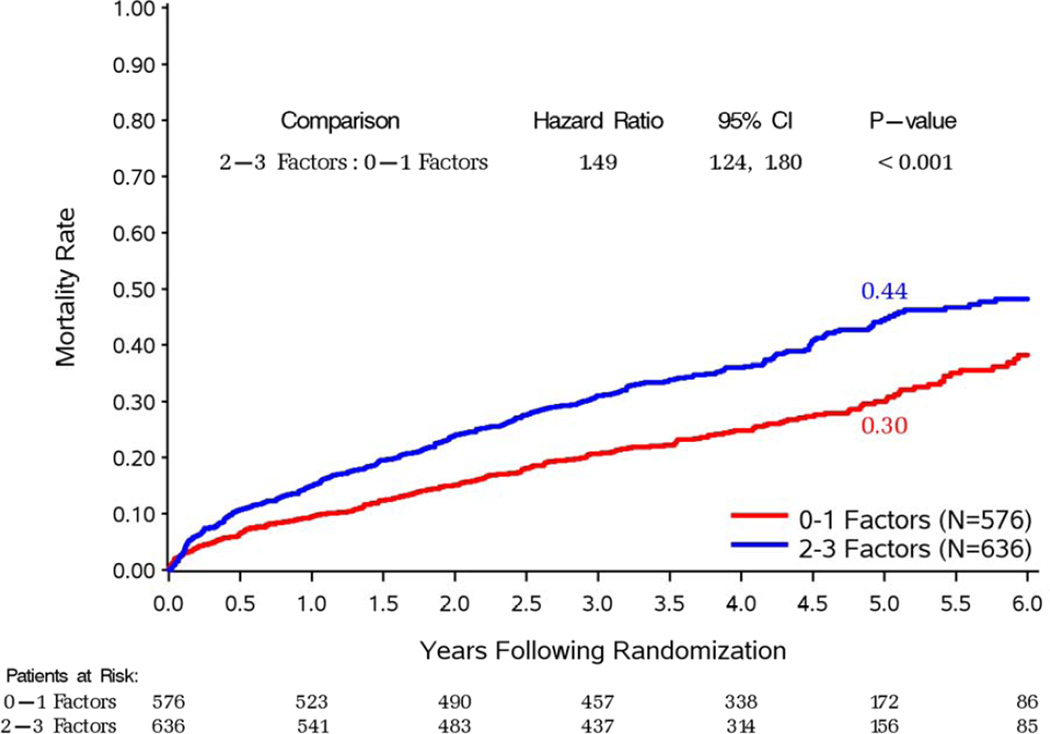
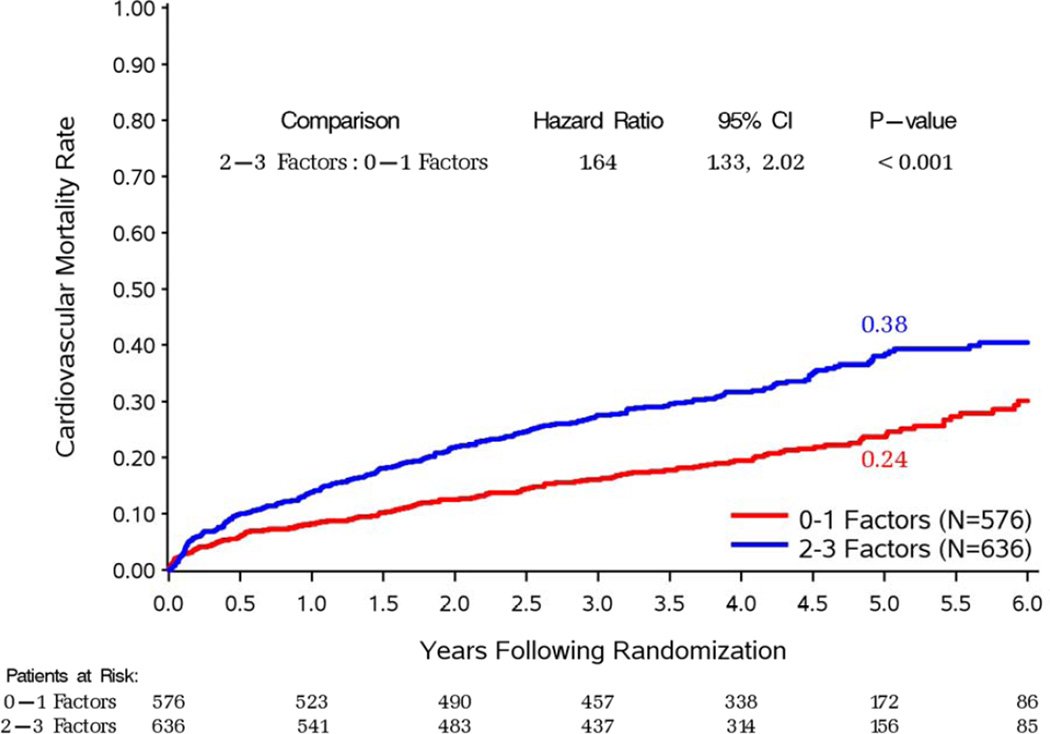
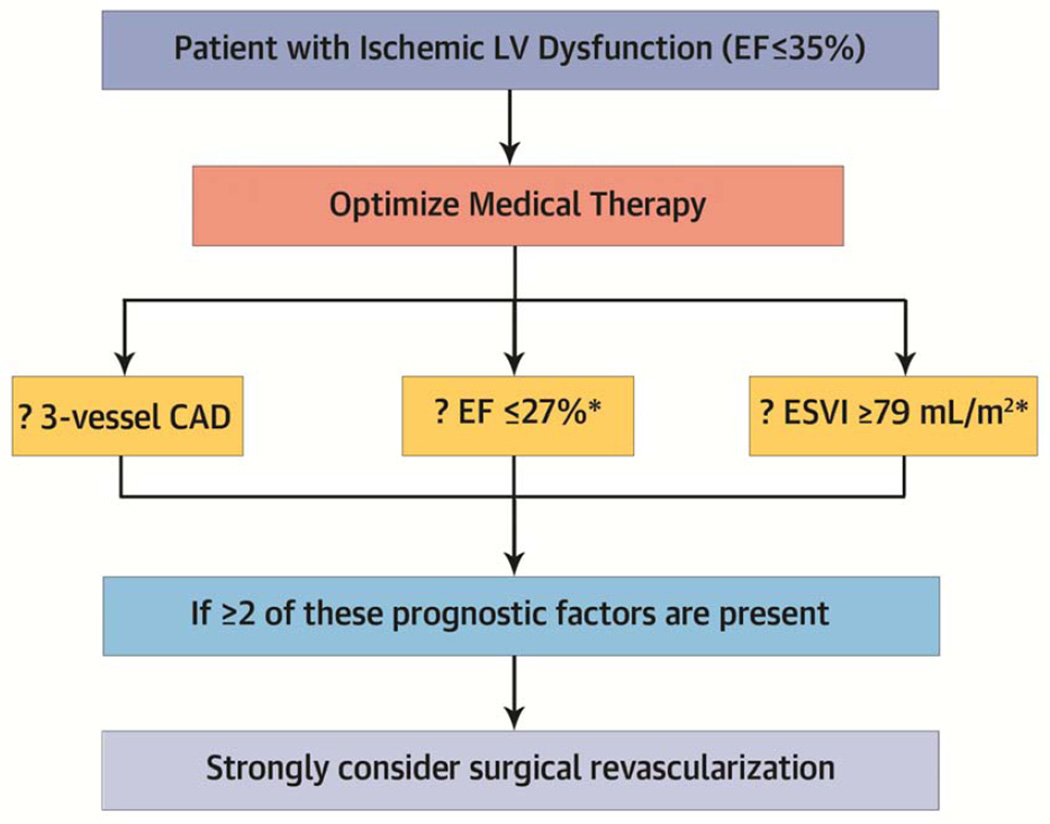
Methods: All 1,212 patients in the STICH (Surgical Treatment of IsChemic Heart failure) surgical revascularization trial were included. Patients had coronary artery disease (CAD) and ejection fraction (EF) of ≤35% and were randomized to receive CABG plus medical therapy or optimal medical therapy (OMT) alone. This study focused on 3 prognostic factors: presence of 3-vessel CAD, EF below the median (27%), and end-systolic volume index (ESVI) above the median (79 ml/m(2)). Patients were categorized as having 0 to 1 or 2 to 3 of these factors.
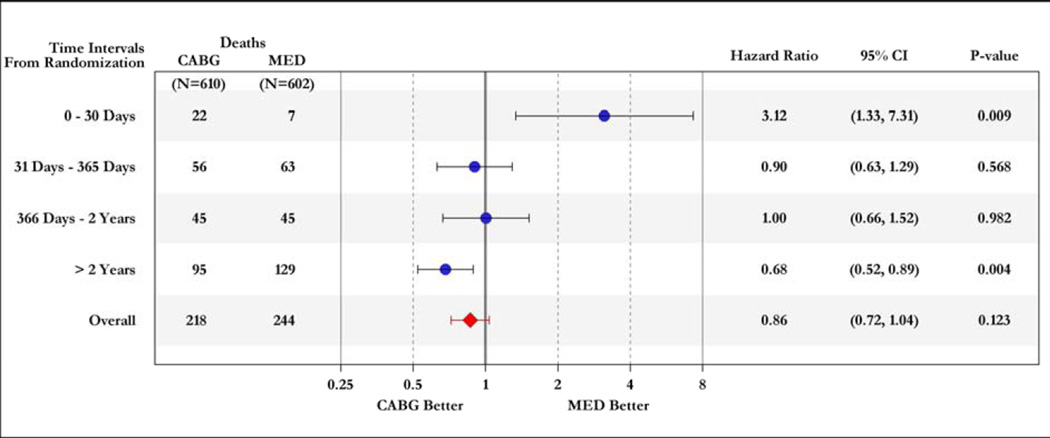
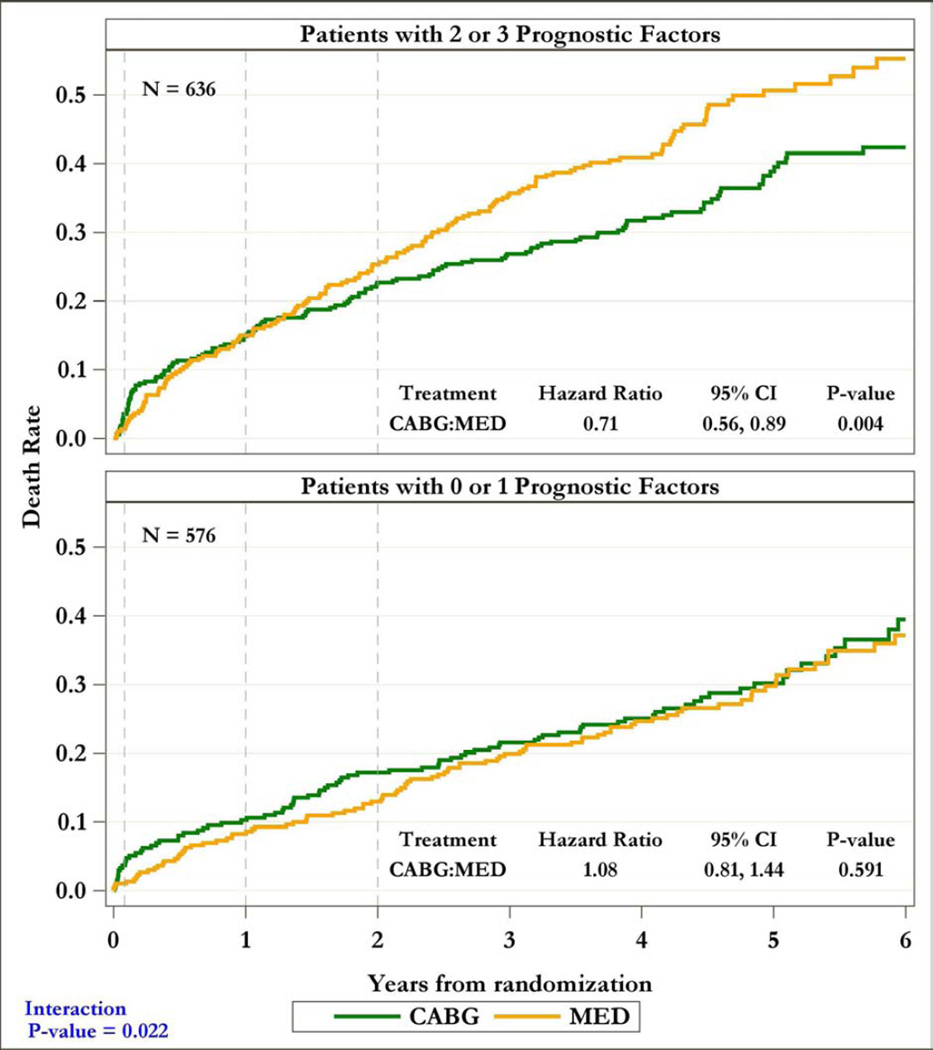
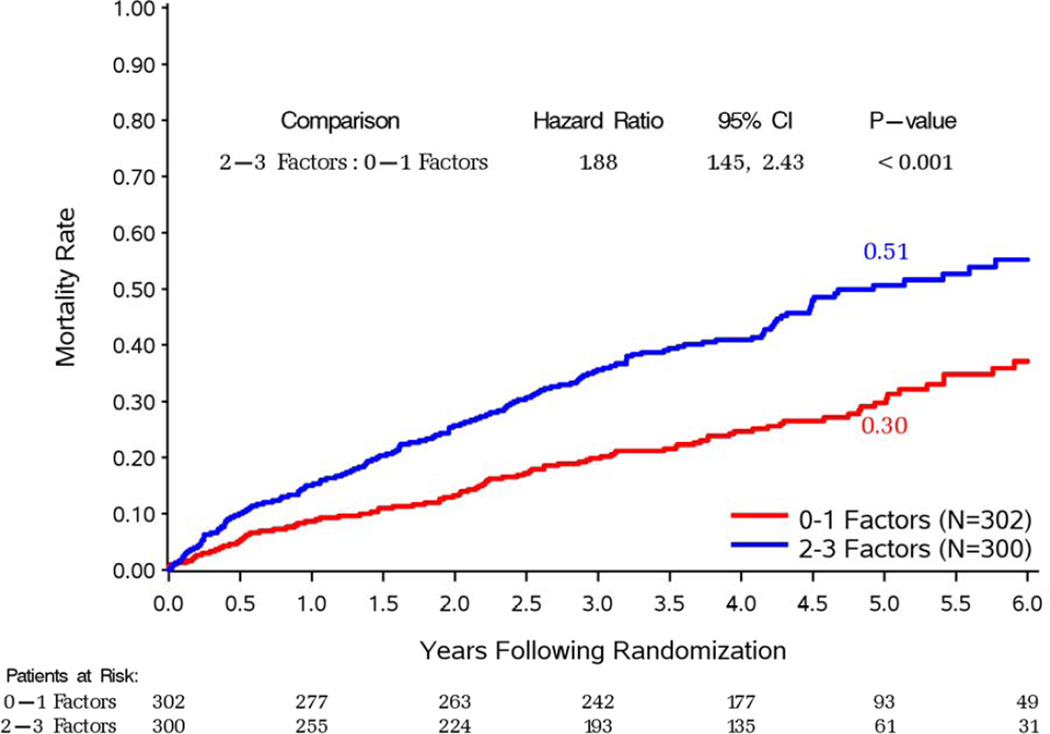
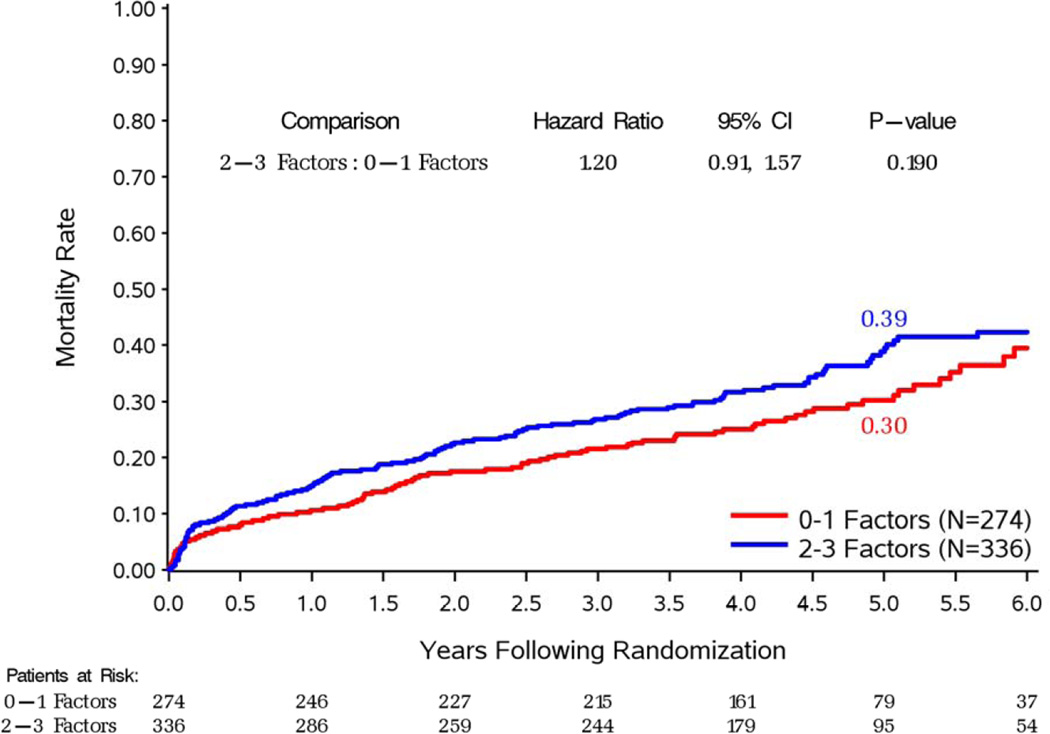
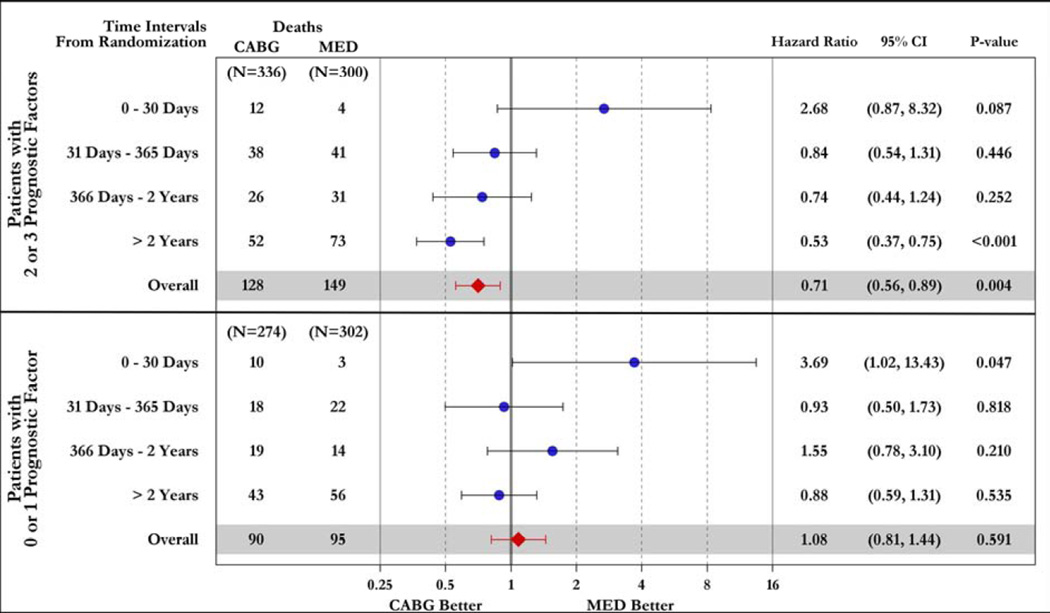
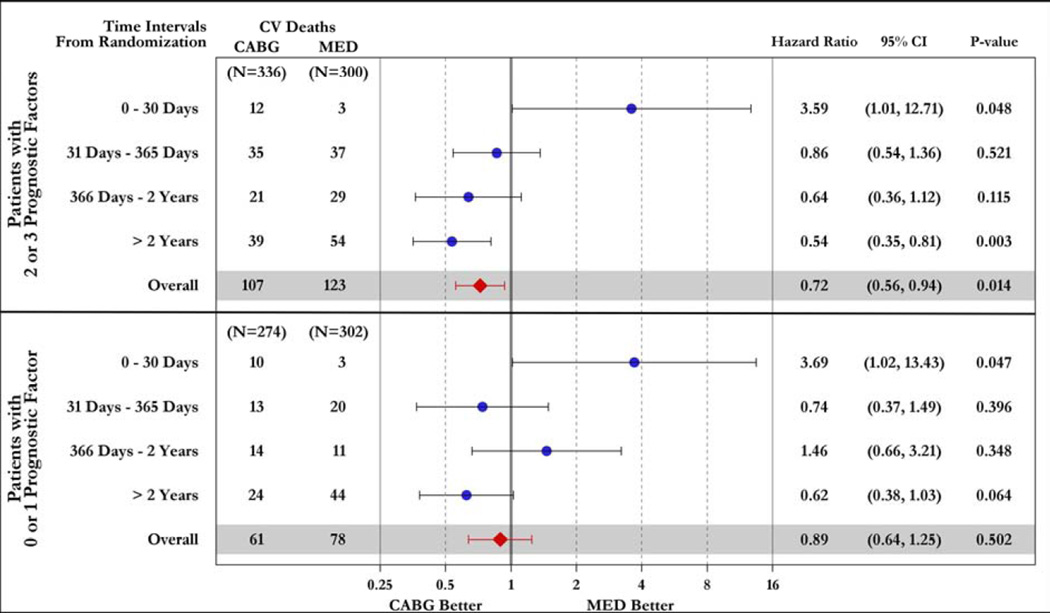
Results: Patients with 2 to 3 prognostic factors (n = 636) had reduced mortality with CABG compared with those who received OMT (hazard ratio [HR]: 0.71; 95% confidence interval [CI]: 0.56 to 0.89; p = 0.004); CABG had no such effect in patients with 0 to 1 factor (HR: 1.08; 95% CI: 0.81 to 1.44; p = 0.591). There was a significant interaction between the number of factors and the effect of CABG on mortality (p = 0.022). Although 30-day risk with CABG was higher, a net beneficial effect of CABG relative to OMT was observed at >2 years in patients with 2 to 3 factors (HR: 0.53; 95% CI: 0.37 to 0.75; p<0.001) but not in those with 0 to 1 factor (HR: 0.88; 95% CI: 0.59 to 1.31; p = 0.535).
Conclusions: Patients with more advanced ischemic cardiomyopathy receive greater benefit from CABG. This supports the indication for surgical revascularization in patients with more extensive CAD and worse myocardial dysfunction and remodeling. (Comparison of Surgical and Medical Treatment for Congestive Heart Failure and Coronary Artery Disease [STICH]; NCT00023595).
Keywords: coronary artery disease; heart failure; left ventricular dysfunction; myocardial ischemia; outcomes.
Copyright © 2014 American College of Cardiology Foundation. Published by Elsevier Inc. All rights reserved.
Figures
Comment in
-
In search of a solution from the STICH trial.J Am Coll Cardiol. 2014 Aug 12;64(6):562-4. doi: 10.1016/j.jacc.2014.05.032. J Am Coll Cardiol. 2014. PMID: 25104524 No abstract available.
References
-
- Serruys PW, Morice MC, Kappetein AP, et al. Percutaneous coronary intervention versus coronary-artery bypass grafting for severe coronary artery disease. N Engl J Med. 2009;360:961–972. - PubMed
-
- Farkouh ME, Domanski M, Sleeper LA, et al. Strategies for multivessel revascularization in patients with diabetes. N Engl J Med. 2012;367:2375–2384. - PubMed
-
- Herlitz J, Karlson BW, Sjoland H, et al. Long term prognosis after CABG in relation to preoperative left ventricular ejection fraction. Int J Cardiol. 2000;72:163–171. - PubMed
-
- Topkara VK, Cheema FH, Kesavaramanujam S, et al. Coronary artery bypass grafting in patients with low ejection fraction. Circulation. 2005;112(suppl I):I344–I350. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
