

Aging and the burden of multimorbidity: associations with inflammatory and anabolic hormonal biomarkers
- PMID: 25104822
- PMCID: PMC4296167
- DOI: 10.1093/gerona/glu127
Aging and the burden of multimorbidity: associations with inflammatory and anabolic hormonal biomarkers
Abstract
Background: Multimorbidity increases with aging, but risk factors beyond age are unknown.
Objective: To investigate the association of inflammatory and anabolic hormonal biomarkers with presence and prospective development of multimorbidity.
Methods: Nine-year longitudinal study of 1018 participants aged 60 years or older (InCHIANTI Study). Multimorbidity was evaluated at baseline and follow-up visits as number of diagnosed diseases from a predefined list of 15 candidate chronic conditions, defined according to standard clinical criteria. Linear mixed models were used to test cross-sectional and longitudinal associations between candidate biomarkers and multimorbidity.
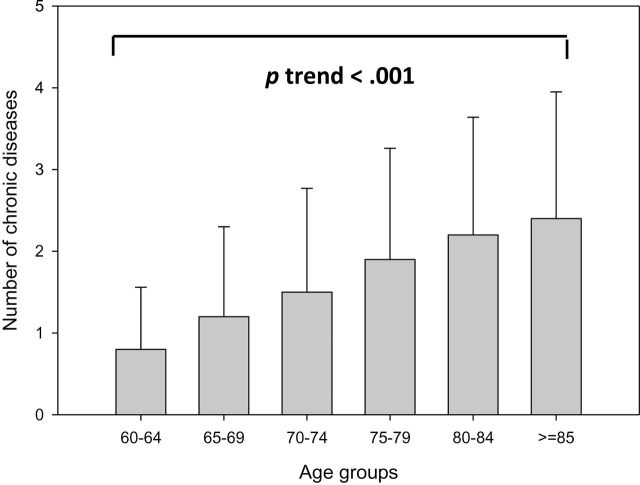
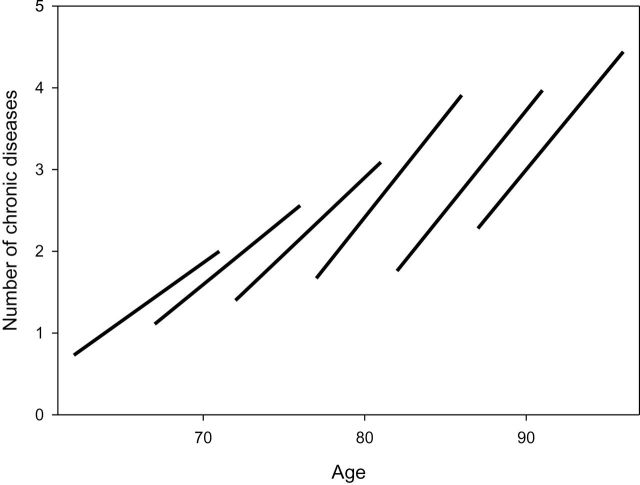
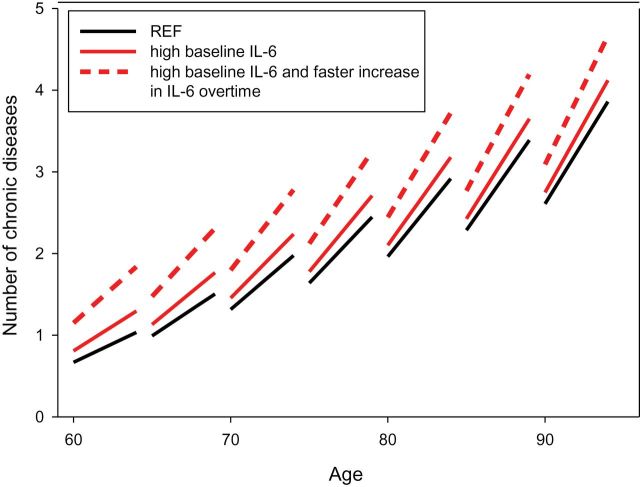
Results: At baseline, multimorbidity was significantly higher in older participants (p < .001) and higher IL-6, IL-1ra, TNF-α receptor II (TNFAR2), and lower dehydroepiandrosterone sulfate were associated with higher number of diseases, independent of age, sex, body mass index, and education. The rate of longitudinal increase in number of chronic diseases was significantly steeper in participants who were older at baseline (p < .001). In addition, higher baseline IL-6 and steeper increase of IL-6 levels were significantly and independently associated with a steeper increase in multimorbidity over time (p < .001 and p = .003, respectively). Sensitivity analyses, performed using 15 different models obtained by removing each of 15 conditions included in the original list of candidate diseases, confirmed that results were not driven by any specific condition.
Conclusions: Accumulation of chronic diseases accelerates at older ages and in persons with higher baseline levels and steeper increase over time of IL-6. High IL-6 and increase in IL-6 may serve as early warning sign to better target interventions aimed at reducing the burden of multimorbidity.
Keywords: Aging; Chronic diseases.; Inflammation; Interleukin-6; Multimorbidity.
Published by Oxford University Press on behalf of the Gerontological Society of America 2014.
Figures
References
-
- Parekh AK, Barton MB. The challenge of multiple comorbidity for the US health care system. JAMA. 2010;303:1303–1304 doi:10.1370/afm.1391 - PubMed
-
- Van den Akker M, Buntinx F, Knottnerus JA. Comorbidity or multimorbidity: what’s in a name? A review of literature. Eur J Gen Pract. 1996;2:65–70.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
