

Does the Risk Assessment and Prediction Tool predict discharge disposition after joint replacement?
- PMID: 25106801
- PMCID: PMC4294888
- DOI: 10.1007/s11999-014-3851-z
Does the Risk Assessment and Prediction Tool predict discharge disposition after joint replacement?
Abstract
Background: Payers of health services and policymakers place a major focus on cost containment in health care. Studies have shown that early planning of discharge is essential in reducing length of stay and achieving financial benefit; tools that can help predict discharge disposition would therefore be of use. The Risk Assessment and Prediction Tool (RAPT) is a preoperative survey constructed to predict discharge disposition after total joint arthroplasty (TJA). The RAPT was developed and tested on a population of Australian patients undergoing joint replacement, but its validity in other populations is unknown. A low RAPT score is reported to indicate a high risk of needing any form of inpatient rehabilitation after TJA, including short-term nursing facilities.
Questions/purposes: This study attempts (1) to assess predictive accuracy of the RAPT on US patients undergoing total hip and knee arthroplasty (THA/TKA); and (2) to determine predictive accuracy of each individual score (1-12).
Methods: Between June 2006 and December 2011, RAPT scores of 3213 patients (1449 THAs; 1764 TKAs) were prospectively captured during the preoperative clinical visit. Scores were stored along with other clinical data, including discharge disposition, in a dedicated database on a secure server. The database was queried by the nursing case manager to retrieve the RAPT scores of all patients captured during this time period. Binary logistic regression was used to analyze the scores and determine predictive accuracy.
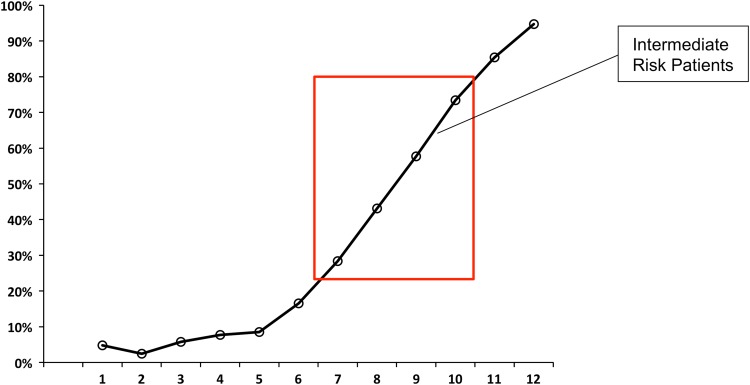
Results: Overall predictive accuracy was 78%. RAPT scores<6 and >10 (of 12) predicted with >90% accuracy discharge to inpatient rehabilitation and home, respectively. Predictive accuracy was lowest for scores between 7 and 10 at 65.2% and almost 50% of patients received scores in this range. Based on our findings, the risk categories in our populations should be high risk<7, intermediate risk 7 to 10, and low risk>10.
Conclusions: The RAPT accurately predicted discharge disposition for high- and low-risk patients in our cohort. Based on our data, intermediate-risk patients should be defined as those with scores of 7 to 10. Predictive accuracy for these patients could potentially be improved through the identification and addition of other factors correlated to discharge disposition. The RAPT allows for identification of patients who are likely to be discharged home or to rehabilitation, which may facilitate preoperative planning of postoperative care. Additionally, it identifies intermediate-risk patients and could be used to implement targeted interventions to facilitate discharge home in this group of patients.
Level of evidence: Level III, diagnostic study. See the Guidelines for Authors for a complete description of levels of evidence.
Figures
Comment in
-
Letter to the Editor: Does the Risk Assessment and Prediction Tool Predict Discharge Disposition After Joint Replacement?Clin Orthop Relat Res. 2015 Nov;473(11):3685-6. doi: 10.1007/s11999-015-4484-6. Epub 2015 Aug 18. Clin Orthop Relat Res. 2015. PMID: 26280682 Free PMC article. No abstract available.
References
-
- Bozic KJ, Katz P, Cisternas M, Ono L, Ries MD, Showstack J. Hospital resource utilization for primary and revision total hip arthroplasty. J Bone Joint Surg Am. 2005;87:570–576. - PubMed
-
- Centers for Disease Control and Prevention. National Hospital Discharge Survey: 2010. Available at: www.cdc.gov/nchs/data/nhds/4procedures/2010pro4_numberprocedureage.pdf. Accessed January 23, 2014.
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
