

Porous metal acetabular components have a low rate of mechanical failure in THA after operatively treated acetabular fracture
- PMID: 25106802
- PMCID: PMC4294918
- DOI: 10.1007/s11999-014-3852-y
Porous metal acetabular components have a low rate of mechanical failure in THA after operatively treated acetabular fracture
Abstract
Background: Total hip arthroplasty (THA) for the treatment of posttraumatic osteoarthritis (OA) after acetabular fracture has been associated with a high likelihood of aseptic loosening, instability, and infection. Porous metal components may help to address the issue of loosening, but there are few data on the use of porous metal acetabular components for posttraumatic OA after acetabular fracture.
Questions/purposes: Using an institutional registry, we aimed to report (1) radiographic evidence of fixation; (2) survivorship free from revision; (3) Harris hip scores; and (4) complications and reoperations after THA with a porous metal acetabular component for posttraumatic OA in patients previously treated with open reduction and internal fixation (ORIF) of a displaced acetabular fracture.
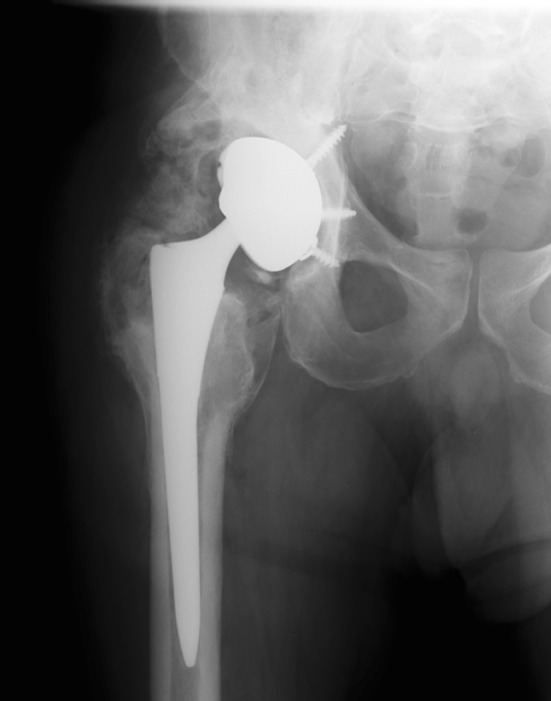
Methods: Thirty primary THAs were performed with a porous metal acetabular component for the treatment of posttraumatic OA after ORIF of an acetabular fracture from 1999 through 2010; of these, 28 (93%) were available for followup at a minimum of 2 years. During that same time, 51 primary THAs were performed using other acetabular designs in patients who had previously undergone ORIF of the acetabulum. During the period in question, the general indications for use of porous metal in this setting included compromised acetabular bone stock or quality to the extent that the treating surgeon believed primary fixation with a titanium shell and screws may have been difficult to achieve. Mean age at the time of arthroplasty was 45 years (range, 23-75 years). Median time from ORIF to THA and from THA to last followup was 107 months (range, 4 months to 42 years) and 60 months (range, 25 months to 10 years), respectively. Radiographs were reviewed for this specific study to evaluate the components for evidence of osteointegration. Survivorship free from revision, hip scores, and complications were extracted from our institutional database and electronic medical record.
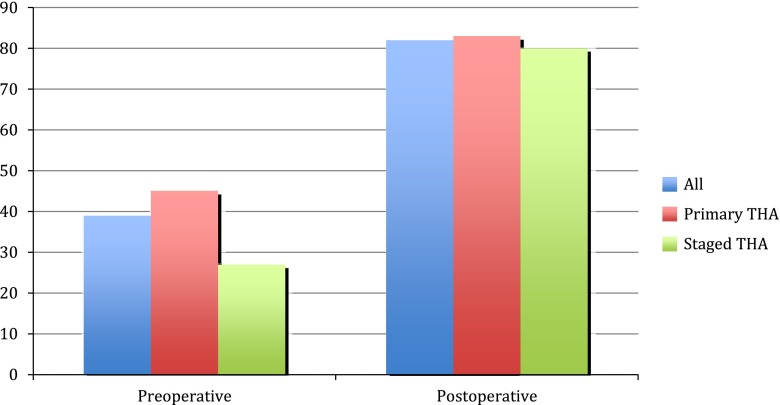
Results: No acetabular or femoral components were revised for aseptic loosening. Five-year survival with revision for any reason as the endpoint was 88% (95% confidence interval, 0.70-0.96). Harris hip scores improved from a median of 39 preoperatively (range, 3-87) to 82 at last followup (range, 21-100; p<0.01). Three hips (11%) underwent resection for infection and all three had been treated with staged arthroplasty for concern of infection. Two patients (7%) experienced at least one dislocation postoperatively.
Conclusions: The short-term results of the use of porous metal acetabular components in THA for treatment of posttraumatic OA after acetabular fracture demonstrate low rates of mechanical failure. Although infection and instability remain major concerns in patients with this diagnosis seemingly regardless of the implant design used, porous metal components appear to offer a high likelihood of osseointegration in this clinical setting.
Level of evidence: Level IV, therapeutic study. See Instructions for Authors for a complete description of levels of evidence.
Figures

References
-
- Berry DJ, Halasy M. Uncemented acetabular components for arthritis after acetabular fracture. Clin Orthop Relat Res. 2002:164–167. - PubMed
-
- Bobyn JD, Poggie RA, Krygier JJ, Lewallen DG, Hanssen AD, Lewis RJ, Unger AS, O’Keefe TJ, Christie MJ, Nasser S, Wood JE, Stulberg SD, Tanzer M. Clinical validation of a structural porous tantalum biomaterial for adult reconstruction. J Bone Joint Surg Am. 2004;86(Suppl 2):123–129. - PubMed
-
- Brooker AF, Bowerman JW, Robinson RA, Riley LH., Jr Ectopic ossification following total hip replacement. Incidence and a method of classification. J Bone Joint Surg Am. 1973;55:1629–1632. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
