

Neutrophil-associated central nervous system inflammation in tuberculous meningitis immune reconstitution inflammatory syndrome
- PMID: 25107295
- PMCID: PMC4227574
- DOI: 10.1093/cid/ciu641
Neutrophil-associated central nervous system inflammation in tuberculous meningitis immune reconstitution inflammatory syndrome
Abstract
Background: The immunopathogenesis of tuberculosis-associated immune reconstitution inflammatory syndrome (IRIS) remains incompletely understood, and we know of only 1 disease site-specific study of the underlying immunology; we recently showed that Mycobacterium tuberculosis culture positivity and increased neutrophils in the cerebrospinal fluid (CSF) of patients with tuberculous meningitis (TBM) are associated with TBM-IRIS. In this study we investigated inflammatory mediators at the disease site in patients with TBM-IRIS.
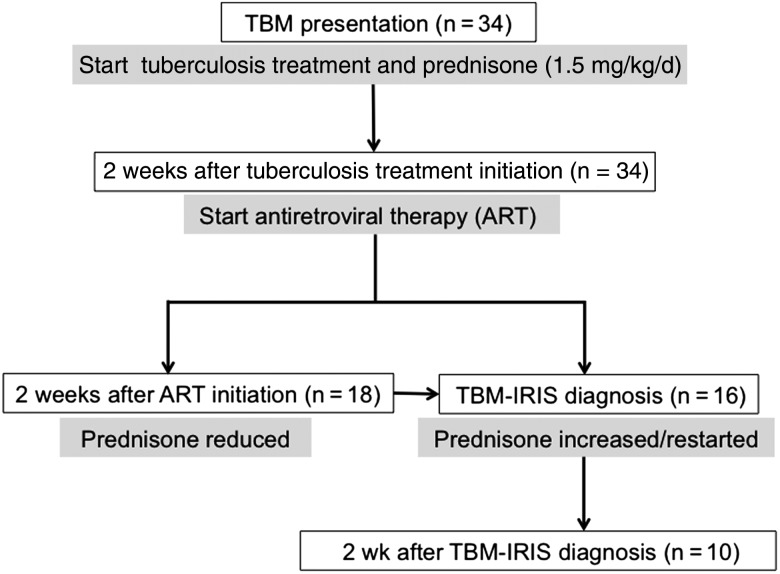
Methods: We performed lumbar puncture at 3-5 time points in human immunodeficiency virus (HIV)-infected patients with TBM (n = 34), including at TBM diagnosis, at initiation of antiretroviral therapy (ART) (day 14), 14 days after ART initiation, at presentation of TBM-IRIS, and 14 days thereafter. We determined the concentrations of 40 mediators in CSF (33 paired with blood) with Luminex or enzyme-linked immunosorbent assays. Findings were compared between patients who developed TBM-IRIS (n = 16) and those who did not (TBM-non-IRIS; n = 18).
Results: At TBM diagnosis and 2 weeks after ART initiation, TBM-IRIS was associated with severe, compartmentalized inflammation in the CSF, with elevated concentrations of cytokines, chemokines, neutrophil-associated mediators, and matrix metalloproteinases, compared with TBM-non-IRIS. Patients with TBM-non-IRIS whose CSF cultures were positive for M. tuberculosis at TBM diagnosis (n = 6) showed inflammatory responses similar to those seen in patients with TBM-IRIS at both time points. However, at 2 weeks after ART initiation, S100A8/A9 was significantly increased in patients with TBM-IRIS, compared with patients with TBM-non-IRIS whose cultures were positive at baseline.
Conclusions: A high baseline M. tuberculosis antigen load drives an inflammatory response that manifests clinically as TBM-IRIS in most, but not all, patients with TBM. Neutrophils and their mediators, especially S100A8/A9, are closely associated with the central nervous system inflammation that characterizes TBM-IRIS.
Keywords: HIV; antiretroviral therapy; therapy-complications; tuberculosis.
© The Author 2014. Published by Oxford University Press on behalf of the Infectious Diseases Society of America.
Figures




References
-
- Burman W, Weis S, Vernon A, et al. Frequency, severity and duration of immune reconstitution events in HIV-related tuberculosis. Int J Tuberc Lung Dis. 2007;11:1282–9. - PubMed
-
- Pepper DJ, Marais S, Maartens G, et al. Neurologic manifestations of paradoxical tuberculosis-associated immune reconstitution inflammatory syndrome: a case series. Clin Infect Dis. 2009;48:e96–107. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
