

Timing of RRT based on the presence of conventional indications
- PMID: 25107952
- PMCID: PMC4152821
- DOI: 10.2215/CJN.12691213
Timing of RRT based on the presence of conventional indications
Abstract
Background and objectives: No data on the development of conventional indications for RRT (refractory acidosis, hyperkalemia, uremia, oliguria/anuria, and volume overload) related to timing of RRT exist. The prevalence of conventional indications among critically ill patients on RRT for AKI was evaluated, and patients manifesting indications versus patients without indications were compared in terms of crude and adjusted 90-day mortality.
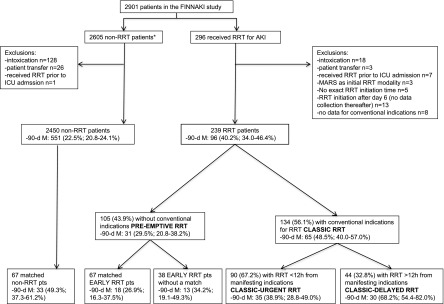
Design, setting, participants, & measurements: In this substudy of the Finnish Acute Kidney Injury study conducted in 2011 and 2012 in 17 intensive care units with 2901 patients, patients were classified as pre-emptive (no conventional indications) and classic (one or more indications) RRT recipients. Patients with classic RRT were divided into classic-urgent (RRT initiated ≤ 12 hours from manifesting indications) and classic-delayed (RRT >12 hours from first indication). Additionally, 2450 patients treated without RRT were matched to patients with pre-emptive RRT.
Results: Of 239 patients treated with RRT, 134 (56.1%; 95% confidence interval [95% CI], 49.8% to 62.4%) fulfilled at least one conventional indication before commencing RRT. Crude 90-day mortality of 134 patients with classic RRT was 48.5% (95% CI, 40.0% to 57.0%), and it was 29.5% (95% CI, 20.8% to 38.2%) for the 105 patients with pre-emptive RRT. Classic RRT was associated with a higher risk for mortality (adjusted odds ratio, 2.05; 95% CI, 1.03 to 4.09). Forty-four patients with classic-delayed RRT showed higher crude mortality (68.2%; 95% CI, 54.4% to 82.0%) compared with patients with classic-urgent RRT, and this association persisted after adjustment for known confounders (odds ratio, 3.85; 95% CI, 1.48 to 10.22). Crude 90-day mortality of 67 1:1 matched patients with pre-emptive RRT was 26.9% (95% CI, 6.3% to 37.5%), and it was 49.3% (95% CI, 37.3% to 61.2%; P=0.01) for their non-RRT matches.
Conclusions: Patients on RRT after one or more conventional indications had both higher crude and adjusted 90-day mortality compared with patients without conventional indications. These findings require confirmation in an adequately powered, multicenter, randomized controlled trial.
Keywords: AKI; RRT; critically ill; indications; timing.
Copyright © 2014 by the American Society of Nephrology.
Figures
Comment in
-
A policy of preemption: the timing of renal replacement therapy in AKI.Clin J Am Soc Nephrol. 2014 Sep 5;9(9):1510-2. doi: 10.2215/CJN.07210714. Epub 2014 Aug 8. Clin J Am Soc Nephrol. 2014. PMID: 25107949 Free PMC article. No abstract available.
References
-
- Kidney Disease: Improving Global Outcomes (KDIGO) Acute Kidney Injury Work Group : KDIGO clinical practice guideline for acute kidney injury. Kidney Int [Suppl]2: 1–138, 2012
-
- Seabra VF, Balk EM, Liangos O, Sosa MA, Cendoroglo M, Jaber BL: Timing of renal replacement therapy initiation in acute renal failure: A meta-analysis. Am J Kidney Dis 52: 272–284, 2008 - PubMed
-
- Bell M, Liljestam E, Granath F, Fryckstedt J, Ekbom A, Martling CR: Optimal follow-up time after continuous renal replacement therapy in actual renal failure patients stratified with the RIFLE criteria. Nephrol Dial Transplant 20: 354–360, 2005 - PubMed
-
- Shiao CC, Wu VC, Li WY, Lin YF, Hu FC, Young GH, Kuo CC, Kao TW, Huang DM, Chen YM, Tsai PR, Lin SL, Chou NK, Lin TH, Yeh YC, Wang CH, Chou A, Ko WJ, Wu KD, National Taiwan University Surgical Intensive Care Unit-Associated Renal Failure Study Group : Late initiation of renal replacement therapy is associated with worse outcomes in acute kidney injury after major abdominal surgery. Crit Care 13: R171, 2009 - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Molecular Biology Databases
