

Advances in clinical management of eosinophilic esophagitis
- PMID: 25109885
- PMCID: PMC4253567
- DOI: 10.1053/j.gastro.2014.07.055
Advances in clinical management of eosinophilic esophagitis
Abstract
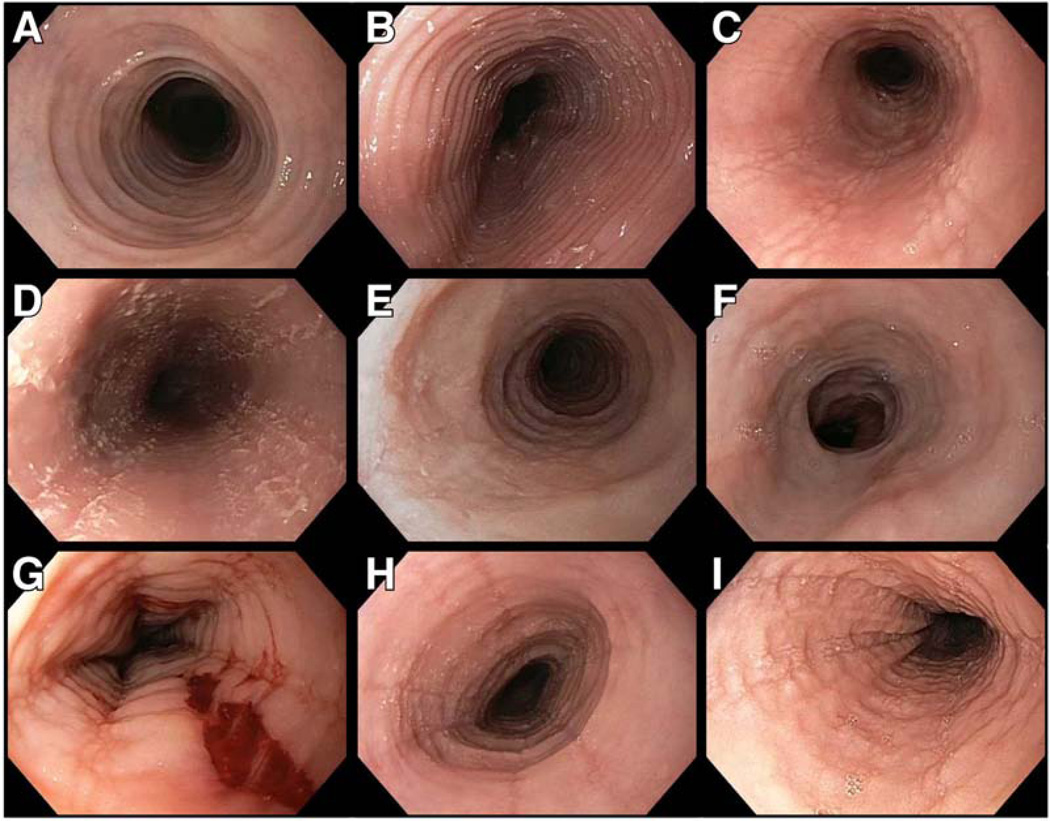
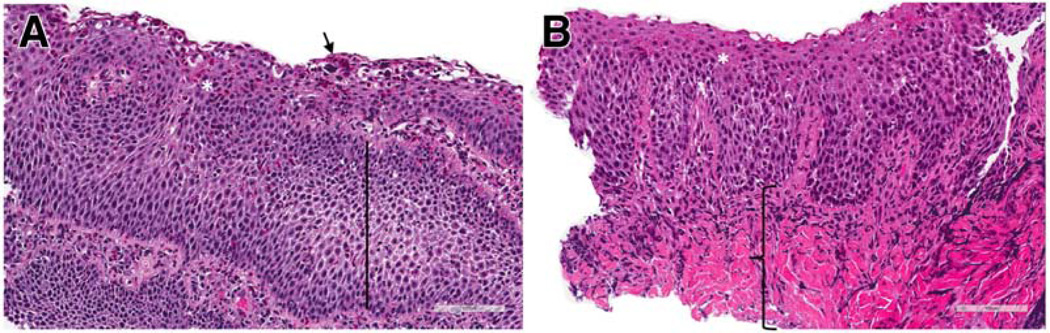
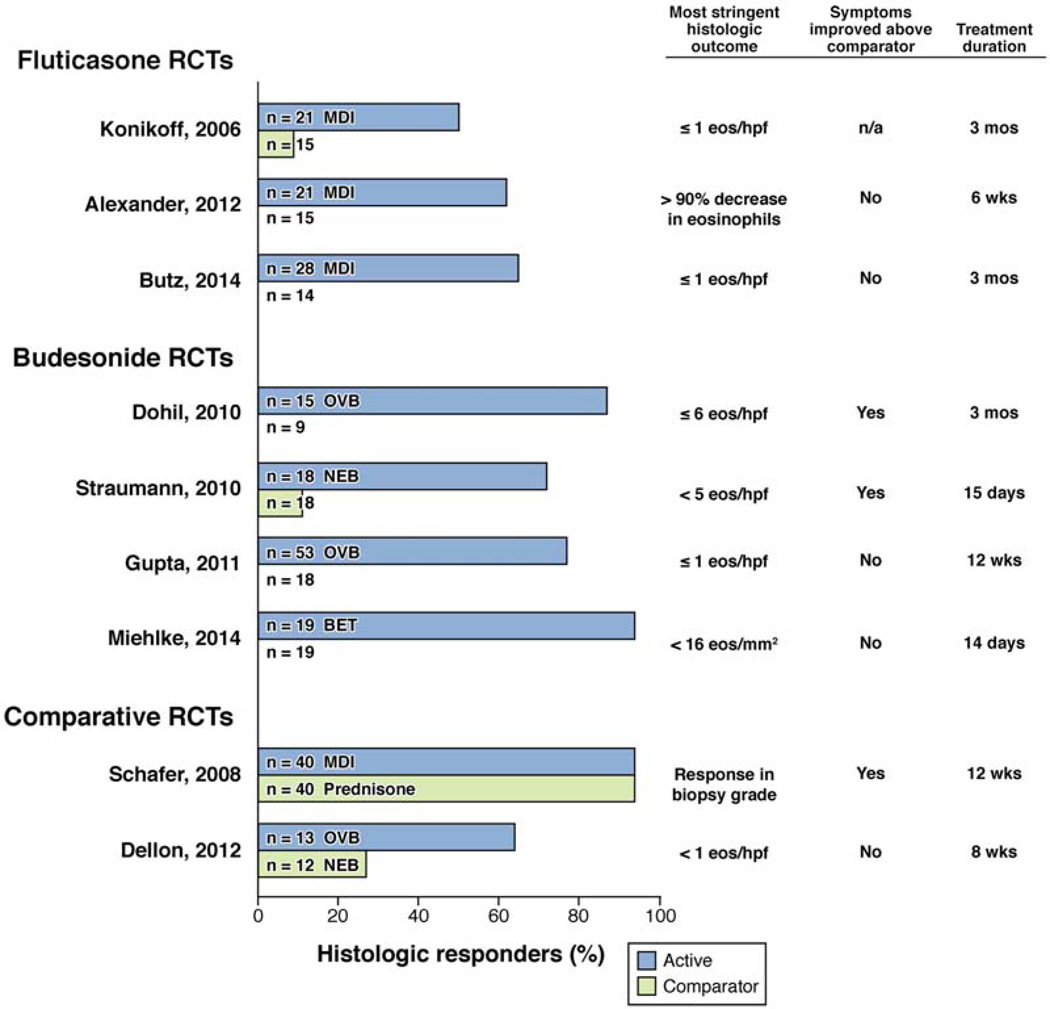
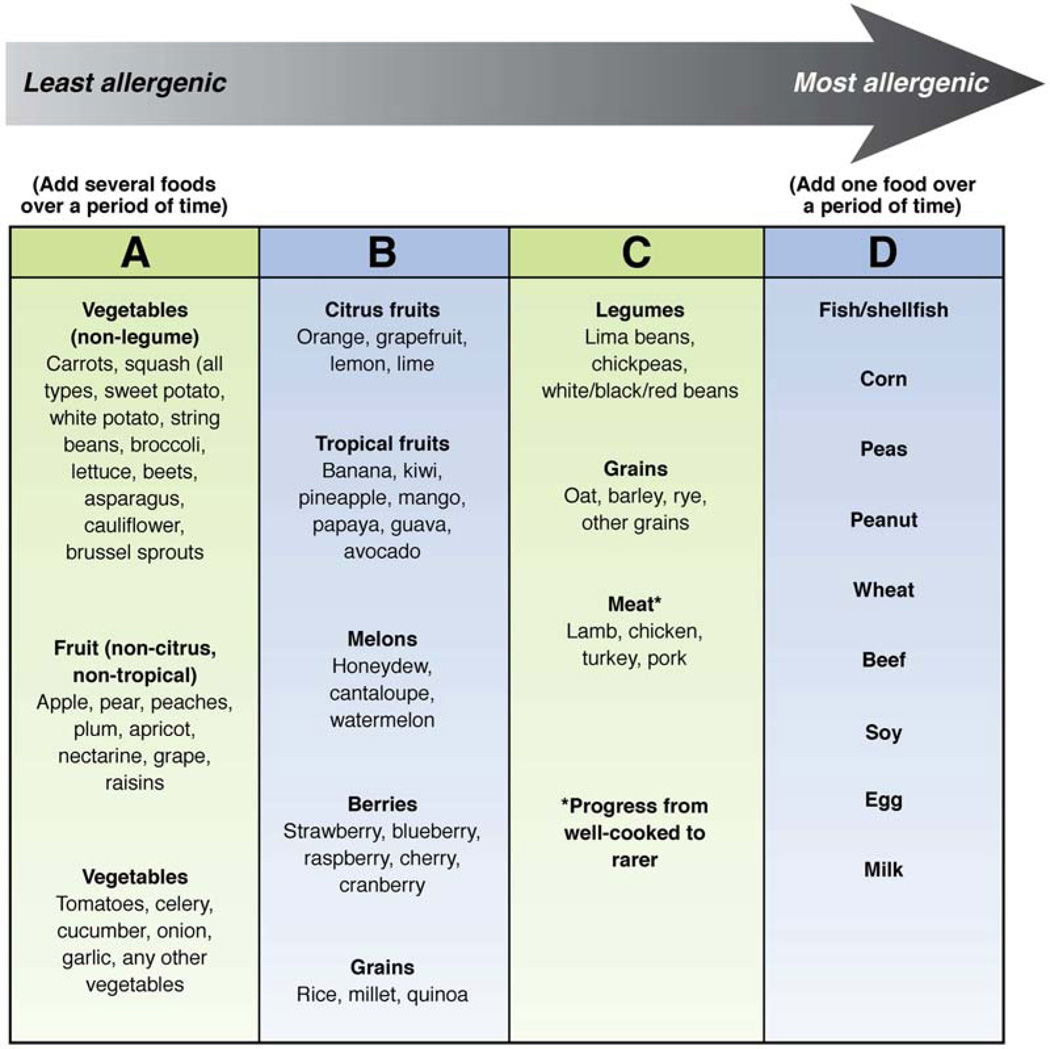
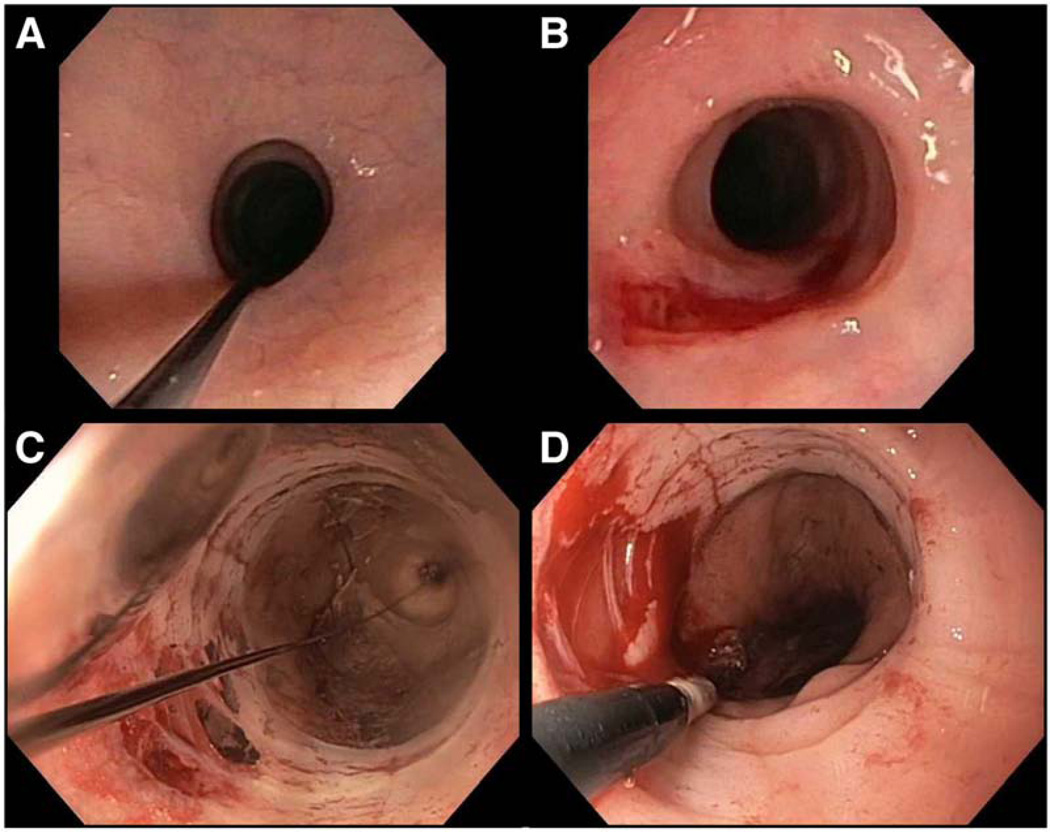
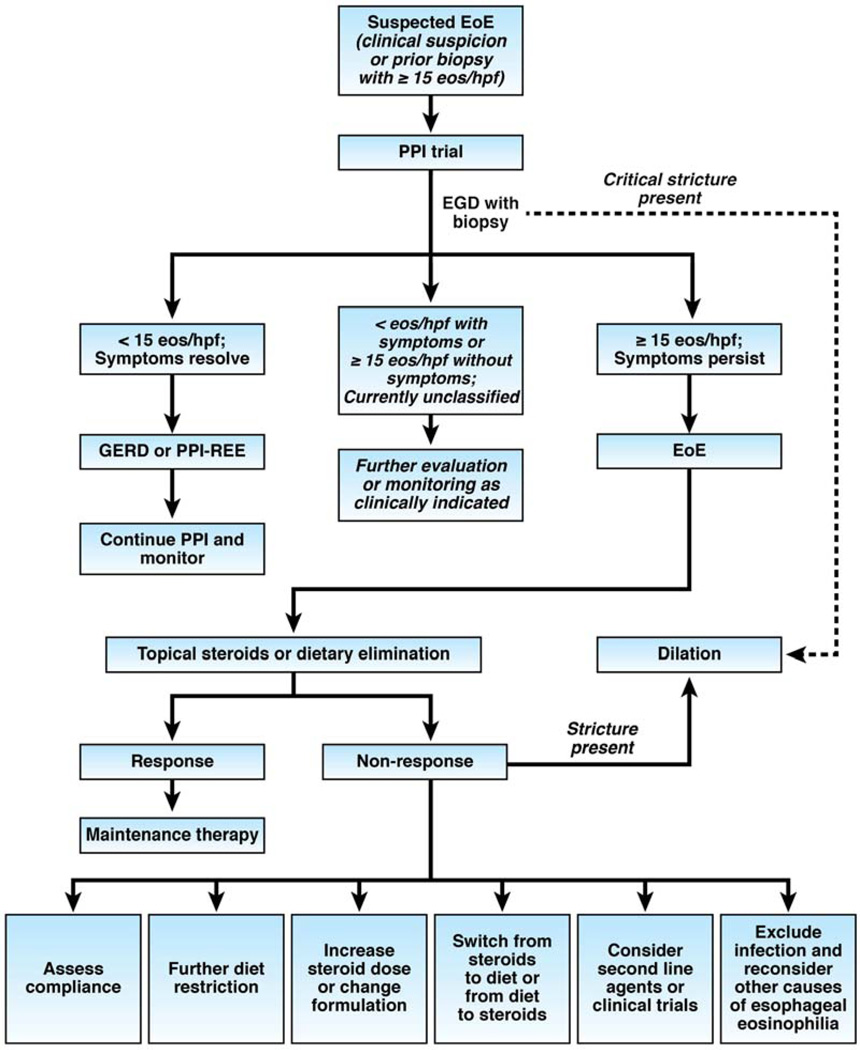
Eosinophilic esophagitis (EoE) is a chronic immune/antigen-mediated clinicopathologic condition that has become an increasingly important cause of upper gastrointestinal morbidity in adults and children over the past 2 decades. It is diagnosed based on symptoms of esophageal dysfunction, the presence of at least 15 eosinophils/high-power field in esophageal biopsy specimens, and exclusion of competing causes of esophageal eosinophilia, including proton pump inhibitor-responsive esophageal eosinophilia. We review what we have recently learned about the clinical aspects of EoE, discussing the clinical, endoscopic, and histological features of EoE in adults and children. We explain the current diagnostic criteria and challenges to diagnosis, including the role of gastroesophageal reflux disease and proton pump inhibitor-responsive esophageal eosinophilia. It is also important to consider the epidemiology of EoE (with a current incidence of 1 new case per 10,000 per year and prevalence of 0.5 to 1 case per 1000 per year) and disease progression. We review the main treatment approaches and new treatment options; EoE can be treated with topical corticosteroids, such as fluticasone and budesonide, or dietary strategies, such as amino acid-based formulas, allergy test-directed elimination diets, and nondirected empiric elimination diets. Endoscopic dilation has also become an important tool for treatment of fibrostenotic complications of EoE. There are a number of unresolved issues in EoE, including phenotypes, optimal treatment end points, the role of maintenance therapy, and treatment of refractory EoE. The care of patients with EoE and the study of the disease span many disciplines; EoE is ideally managed by a multidisciplinary team of gastroenterologists, allergists, pathologists, and dieticians.
Keywords: Diagnosis; Endoscopy; Management Algorithm; Treatment.
Copyright © 2014 AGA Institute. Published by Elsevier Inc. All rights reserved.
Figures
References
-
- Furuta GT, Liacouras CA, Collins MH, Gupta SK, Justinich C, Putnam PE, Bonis P, Hassall E, Straumann A, Rothenberg ME. Eosinophilic esophagitis in children and adults: a systematic review and consensus recommendations for diagnosis and treatment. Gastroenterology. 2007;133:1342–1363. - PubMed
-
- Liacouras CA, Furuta GT, Hirano I, Atkins D, Attwood SE, Bonis PA, Burks AW, Chehade M, Collins MH, Dellon ES, Dohil R, Falk GW, Gonsalves N, Gupta SK, Katzka DA, Lucendo AJ, Markowitz JE, Noel RJ, Odze RD, Putnam PE, Richter JE, Romero Y, Ruchelli E, Sampson HA, Schoepfer A, Shaheen NJ, Sicherer SH, Spechler S, Spergel JM, Straumann A, Wershil BK, Rothenberg ME, Aceves SS. Eosinophilic esophagitis: Updated consensus recommendations for children and adults. J Allergy Clin Immunol. 2011;128:3–20. e6. - PubMed
-
- Dellon ES, Gonsalves N, Hirano I, Furuta GT, Liacouras C, Katzka DA. ACG Clinical Guideline: Evidence based approach to the diagnosis and management of esophageal eosinophilia and eosinophilic esophagitis. Am J Gastroenterol. 2013;108:679–692. - PubMed
-
- Winter HS, Madara JL, Stafford RJ, Grand RJ, Quinlan JE, Goldman H. Intraepithelial eosinophils: a new diagnostic criterion for reflux esophagitis. Gastroenterology. 1982;83:818–823. - PubMed
-
- Attwood SE, Smyrk TC, Demeester TR, Jones JB. Esophageal eosinophilia with dysphagia. A distinct clinicopathologic syndrome. Dig Dis Sci. 1993;38:109–116. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
