

Enoxaparin prevents steroid-related avascular necrosis of the femoral head
- PMID: 25110730
- PMCID: PMC4106066
- DOI: 10.1155/2014/347813
Enoxaparin prevents steroid-related avascular necrosis of the femoral head
Erratum in
-
Corrigendum to "Enoxaparin Prevents Steroid-Related Avascular Necrosis of the Femoral Head".ScientificWorldJournal. 2015;2015:264241. doi: 10.1155/2015/264241. Epub 2015 Aug 26. ScientificWorldJournal. 2015. PMID: 26347899 Free PMC article. No abstract available.
Abstract
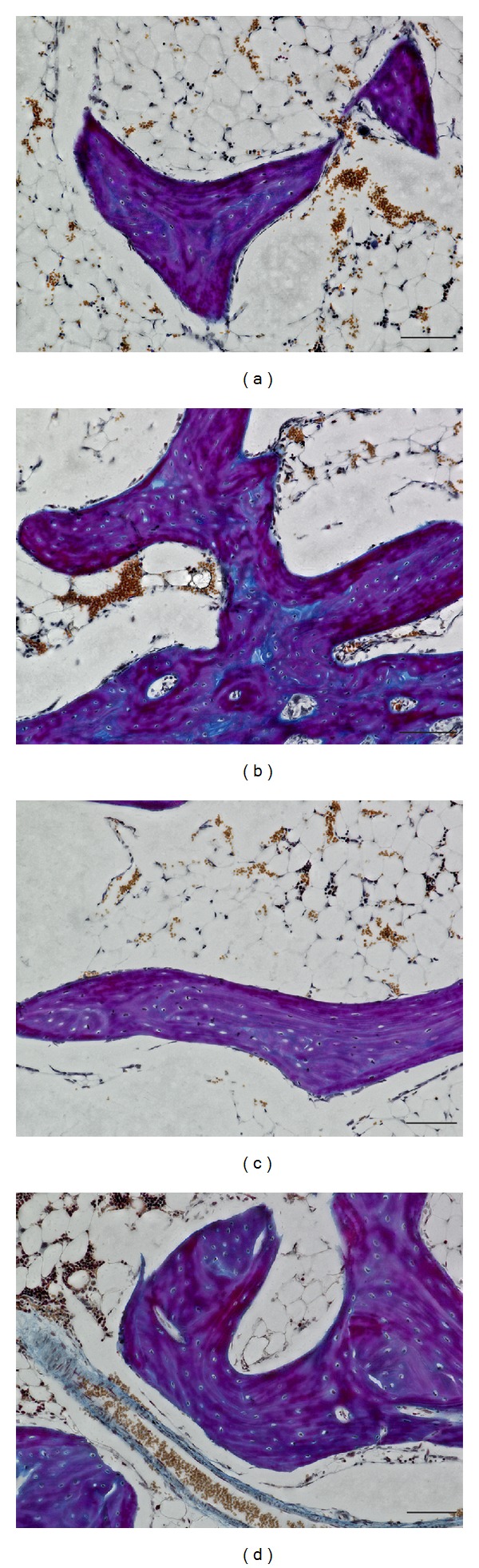
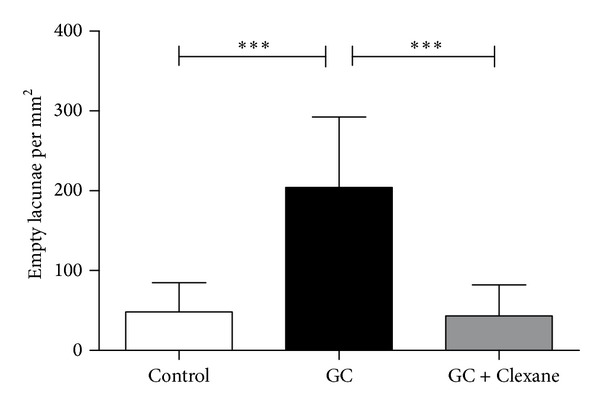
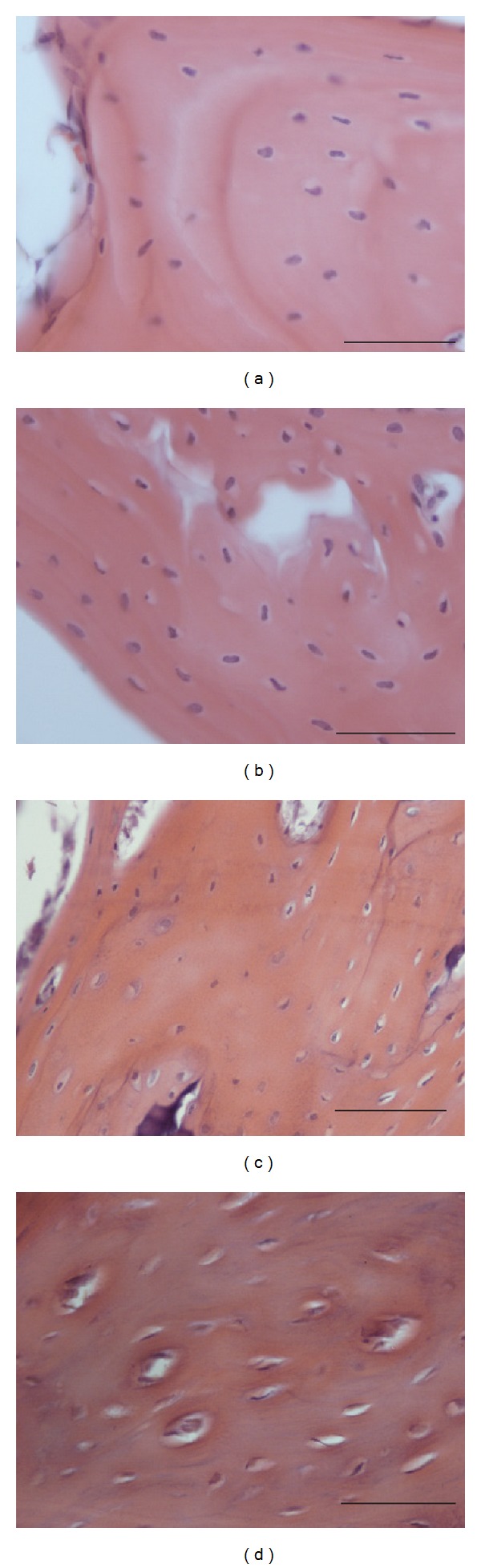
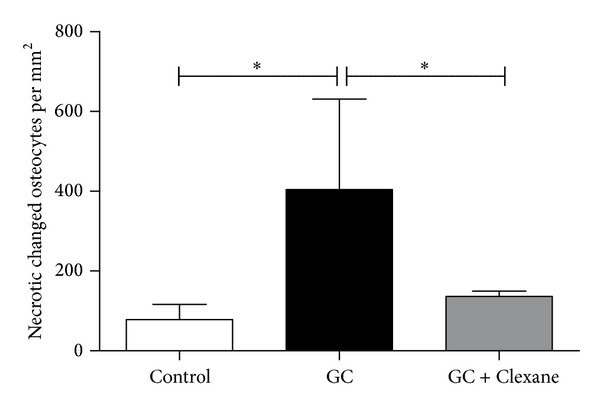
Nontraumatic osteonecrosis of the femoral head is still a challenging problem in orthopedic surgery. It is responsible for 10% of the 500,000 hip replacement surgeries in the USA and affects relatively young, active patients in particular. Main reasons for nontraumatic osteonecrosis are glucocorticoid use, alcoholism, thrombophilia, and hypofibrinolysis (Glueck et al., 1997; Orth and Anagnostakos, 2013). One pathomechanism of steroid-induced osteonecrosis is thought to be impaired blood flow to the femoral head caused by increased thrombus formation and vasoconstriction. To investigate the preventive effect of enoxaparin on steroid-related osteonecrosis, we used male New Zealand white rabbits. Osteonecrosis was induced by methylprednisolone-injection (1 × 20 mg/kg body weight). Control animals were treated with phosphate-buffered saline. Treatment consisted of an injection of 11.7 mg/kg body weight of enoxaparin per day (Clexane) in addition to methylprednisolone. Four weeks after methylprednisolone-injection the animals were sacrificed. Histology (hematoxylin-eosin and Ladewig staining) was performed, and empty lacunae and histological signs of osteonecrosis were quantified. Histomorphometry revealed a significant increase in empty lacunae and necrotic changed osteocytes in glucocorticoid-treated animals as compared with the glucocorticoid- and Clexane-treated animals and with the control group. No significant difference was detected between the glucocorticoid and Clexane group and the control group. This finding suggests that cotreatment with enoxaparin has the potential to prevent steroid-associated osteonecrosis.
Figures
Similar articles
-
Nitrate patch prevents steroid-related bone necrosis.J Orthop Res. 2011 Oct;29(10):1517-20. doi: 10.1002/jor.21420. Epub 2011 Apr 5. J Orthop Res. 2011. PMID: 21469180
-
Combined Treatment with an Anticoagulant and a Vasodilator Prevents Steroid-Associated Osteonecrosis of Rabbit Femoral Heads by Improving Hypercoagulability.Biomed Res Int. 2017;2017:1624074. doi: 10.1155/2017/1624074. Epub 2017 Oct 19. Biomed Res Int. 2017. PMID: 29201897 Free PMC article.
-
[Experimental study on avascular necrosis of femoral head induced by methylprednisolone combined with lipopolysaccharide in rabbits].Zhongguo Xiu Fu Chong Jian Wai Ke Za Zhi. 2008 Mar;22(3):265-70. Zhongguo Xiu Fu Chong Jian Wai Ke Za Zhi. 2008. PMID: 18396700 Chinese.
-
Studies of nontraumatic osteonecrosis. Manometric and histologic studies of the femoral head after chronic steroid treatment: an experimental study in rabbits.Clin Orthop Relat Res. 1987 Dec;(225):128-40. Clin Orthop Relat Res. 1987. PMID: 3315374 Review.
-
The pathogenesis of steroid-induced osteonecrosis of the femoral head: A systematic review of the literature.Gene. 2018 Sep 10;671:103-109. doi: 10.1016/j.gene.2018.05.091. Epub 2018 May 30. Gene. 2018. PMID: 29859289
Cited by
-
Spontaneous bone infarction of the distal femur in a patient with Cushing's disease: a case report.Bone Rep. 2021 Feb 18;14:100756. doi: 10.1016/j.bonr.2021.100756. eCollection 2021 Jun. Bone Rep. 2021. PMID: 33665239 Free PMC article.
-
Downregulated SOX9 mediated by miR-206 promoted cell apoptosis in Legg-Calvé-Perthes disease.Oncol Lett. 2018 Jan;15(1):1319-1324. doi: 10.3892/ol.2017.7373. Epub 2017 Nov 8. Oncol Lett. 2018. PMID: 29387248 Free PMC article.
-
Association of reduced sclerostin expression with collapse process in patients with osteonecrosis of the femoral head.Int Orthop. 2018 Jul;42(7):1675-1682. doi: 10.1007/s00264-018-3979-7. Epub 2018 May 21. Int Orthop. 2018. PMID: 29785591
-
Case report: primary osteonecrosis associated with thrombophilia-hypofibrinolysis and worsened by testosterone therapy.BMC Hematol. 2017 Mar 27;17:5. doi: 10.1186/s12878-017-0076-x. eCollection 2017. BMC Hematol. 2017. PMID: 28361003 Free PMC article.
-
Comparison of the prophylactic use of ibandronate and its use in early-stage osteonecrosis in rats with steroid-induced osteonecrosis of the femoral head.Jt Dis Relat Surg. 2023 Aug 21;34(3):640-650. doi: 10.52312/jdrs.2023.1096. Jt Dis Relat Surg. 2023. PMID: 37750269 Free PMC article.
References
-
- Mont MA, Jones LC, Hungerford DS. Current concepts review—nontraumatic osteonecrosis of the femoral head: ten years later. Journal of Bone and Joint Surgery A. 2006;88(5):1117–1132. - PubMed
-
- Mont MA, Hungerford DS. Non-traumatic avascular necrosis of the femoral head. Journal of Bone and Joint Surgery A. 1995;77(3):459–474. - PubMed
-
- Orth P, Anagnostakos K. Coagulation abnormalities in osteonecrosis and bone marrow edema syndrome. Orthopedics. 2013;36(4):290–300. - PubMed
-
- Motomura G, Yamamoto T, Miyanishi K, Yamashita A, Sueishi K, Iwamoto Y. Bone marrow fat-cell enlargement in early steroid-induced osteonecrosis—a histomorphometric study of autopsy cases. Pathology Research and Practice. 2005;200(11-12):807–811. - PubMed
-
- Glueck CJ, Freiberg R, Tracy T, Stroop D, Wang P. Thrombophilia and hypofibrinolysis: Pathophysiologies of osteonecrosis. Clinical Orthopaedics and Related Research. 1997;(334):43–56. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
