

Coronary artery spasm: An often overlooked diagnosis
- PMID: 25114375
- PMCID: PMC4124553
- DOI: 10.4103/0300-1652.137231
Coronary artery spasm: An often overlooked diagnosis
Abstract
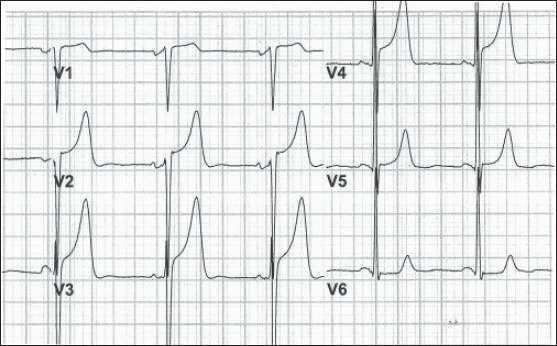
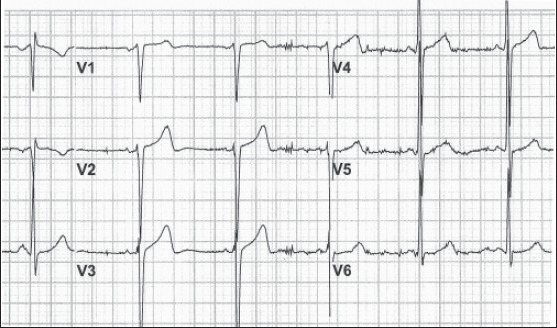
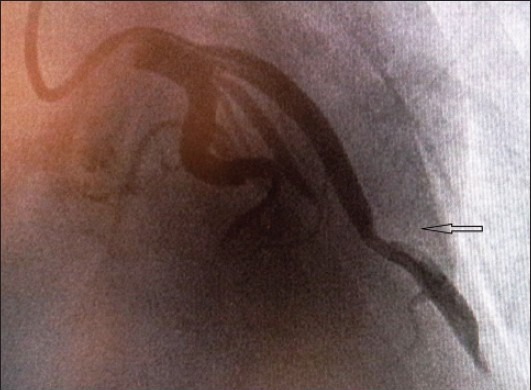
Coronary vasospasm can lead to myocardial injury and even sudden cardiac death. It has generally been overlooked as a diagnosis since atherosclerosis is a more common cause of acute coronary syndromes and because of the dilemma involved in its diagnosis. A middle-aged man with a history of smoking and cocaine use presented to the emergency department with left-sided arm/chest discomfort and diaphoresis. The electrocardiogram showed anterior ST elevation and hyper-acute T waves, which completely resolved shortly after sublingual nitroglycerin was administered. Subsequent angiogram revealed a 70% focal stenosis in the mid-left anterior descending artery. Coronary vasospasm occurs more commonly in arteries with underlying atheromatous disease, although normal vessels are not excluded. Cigarette smoking and cocaine use are among the major culprits that have been implicated as risk factors for the occurrence of coronary vasospasm. Eventually, the patient had percutaneous coronary intervention of his left-anterior descending artery and remained asymptomatic.
Keywords: Angina; coronary; prinzmental; vasospasm.
Conflict of interest statement
Figures
Similar articles
-
Vasospastic Angina Unmasked on Repeat Coronary Angiography in a Patient Without Typical Triggers: A Case Report.Cureus. 2025 Mar 25;17(3):e81139. doi: 10.7759/cureus.81139. eCollection 2025 Mar. Cureus. 2025. PMID: 40276394 Free PMC article.
-
A Rare Case of Vasospasm Presenting with Acute Coronary Syndrome and Leading to Total Occlusion.Turk Kardiyol Dern Ars. 2023 Sep;51(6):415-418. doi: 10.5543/tkda.2023.73858. Turk Kardiyol Dern Ars. 2023. PMID: 37671515 English.
-
Marijuana-induced Coronary Vasospasm with Persistent Inter-coronary Connection: A Case Report and Review of Literature.Cureus. 2019 Jun 1;11(6):e4799. doi: 10.7759/cureus.4799. Cureus. 2019. PMID: 31497413 Free PMC article.
-
Recurrent myocardial infarction secondary to Prinzmetal's variant angina.Singapore Med J. 2015 May;56(5):e74-7. doi: 10.11622/smedj.2015077. Singapore Med J. 2015. PMID: 26034323 Free PMC article.
-
Vasospastic Angina Presenting With Syncope and Chest Pain: A Case Report and Brief Literature Review.S D Med. 2017 Nov;70(11):498-502. S D Med. 2017. PMID: 29088521 Review.
Cited by
-
ST elevation in recovery post exercise with normal coronary arteries.BMJ Case Rep. 2019 Jul 8;12(7):e229766. doi: 10.1136/bcr-2019-229766. BMJ Case Rep. 2019. PMID: 31289167 Free PMC article.
-
Life-Threatening Coronary Vasospasm Treated by Implantable Cardioverter Defibrillator: The Warning Signs.Case Rep Cardiol. 2022 Jul 27;2022:4504028. doi: 10.1155/2022/4504028. eCollection 2022. Case Rep Cardiol. 2022. PMID: 35937136 Free PMC article.
-
Acute and Chronic Effects of Cocaine on Cardiovascular Health.Int J Mol Sci. 2019 Jan 29;20(3):584. doi: 10.3390/ijms20030584. Int J Mol Sci. 2019. PMID: 30700023 Free PMC article. Review.
-
Pannus-related prosthetic valve dysfunction. Case report.Clujul Med. 2016;89(1):169-75. doi: 10.15386/cjmed-510. Epub 2016 Jan 15. Clujul Med. 2016. PMID: 27004041 Free PMC article.
-
Coronary vasospasm complicating atrial fibrillation ablation: a case report and review of the literature.J Community Hosp Intern Med Perspect. 2020 Aug 2;10(4):346-349. doi: 10.1080/20009666.2020.1774252. J Community Hosp Intern Med Perspect. 2020. PMID: 32850095 Free PMC article.
References
-
- Prinzmetal M, Kennamer R, Merliss R, Wada T, Bor N, Angina pectoris I. A variant form of angina pectoris; preliminary report. Am J Med Sci. 1959;27:375–88. - PubMed
-
- Mishra PK. Variations in presentation and various options in management of variant angina. Eur J Cardiothoracic Surg. 2006;29:748–59. - PubMed
-
- Antman EM, Anbe DT, Armstrong PW, Bates ER, Green LA, Hand M, et al. American College of Cardiology, American Heart Association Task Force on Practice Guidelines, Canadian Cardiovascular Society. ACC/AHA guidelines for the management of patients with ST-elevation myocardial infarction: A report of the American College ofCardiology/American Heart Association Task Force on Practice Guidelines (Committee to Revise the 1999 Guidelines for the Management of Patients with Acute Myocardial Infarction) Circulation. 2004;110:e82–292. - PubMed
-
- Maseri A, Davies G, Hackett D, Kaski JC. Coronary artery spasm and vasoconstriction. The case for a distinction. Circulation. 1990;81:1983–91. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
