Early initiation of prophylactic heparin in severe traumatic brain injury is associated with accelerated improvement on brain imaging
- PMID: 25114421
- PMCID: PMC4126111
- DOI: 10.4103/0974-2700.136846
Early initiation of prophylactic heparin in severe traumatic brain injury is associated with accelerated improvement on brain imaging
Abstract
Background: Venous thromboembolic prophylaxis (VTEp) is often delayed following traumatic brain injury (TBI), yet animal data suggest that it may reduce cerebral inflammation and improve cognitive recovery. We hypothesized that earlier VTEp initiation in severe TBI patients would result in more rapid neurologic recovery and reduced progression of brain injury on radiologic imaging.
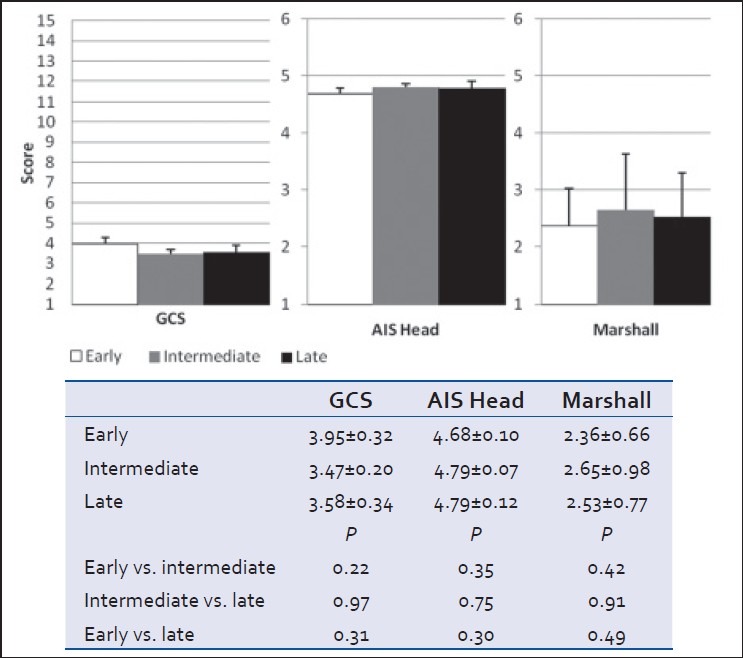
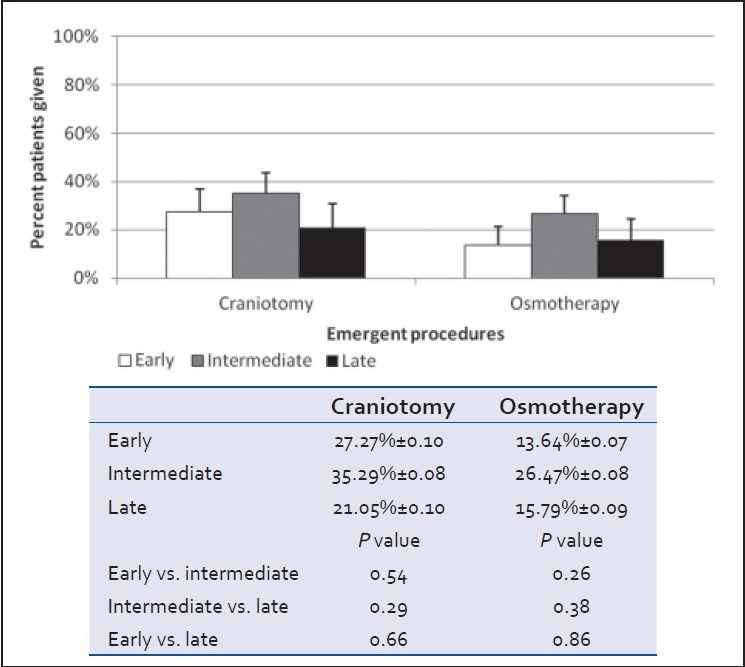
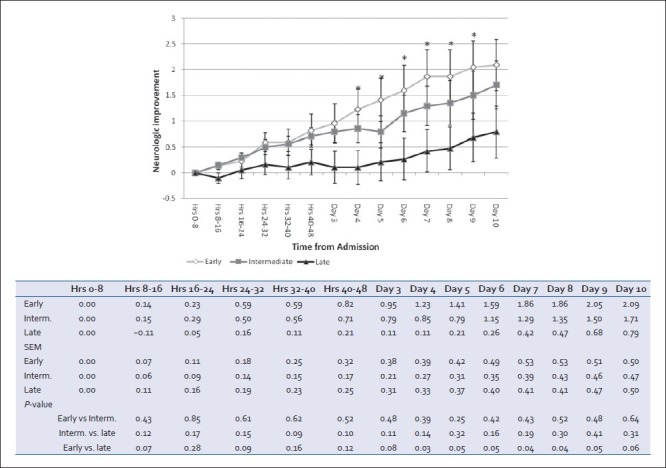
Study design: Medical charts of severe TBI patients admitted to a level 1 trauma center in 2009-2010 were queried for admission Glasgow Coma Scale (GCS), head Abbreviated Injury Scale, Injury Severity Score (ISS), osmotherapy use, emergency neurosurgery, and delay to VTEp initiation. Progression (+1 = better, 0 = no change, -1 = worse) of brain injury on head CTs and neurologic exam (by bedside MD, nurse) was collected from patient charts. Head CT scan Marshall scores were calculated from the initial head CT results.
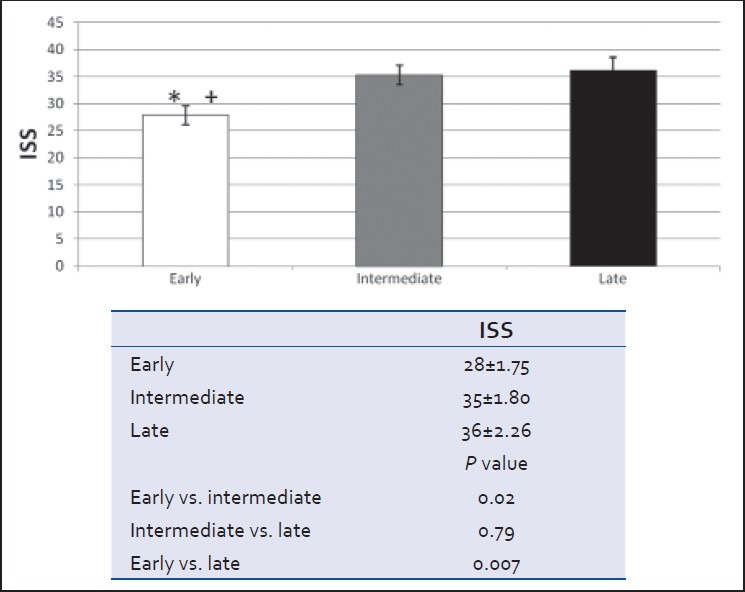
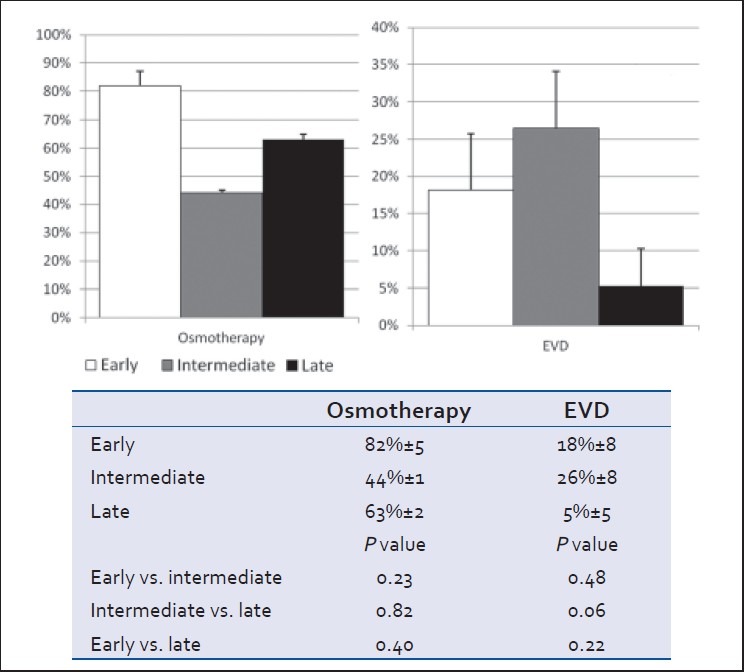
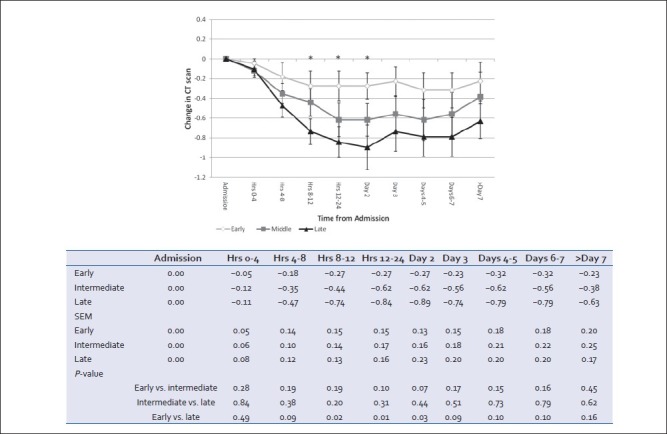
Results: A total of 22, 34, and 19 patients received VTEp at early (<3 days), intermediate (3-5 days), and late (>5 days) time intervals, respectively. Clinical and radiologic brain injury characteristics on admission were similar among the three groups (P > 0.05), but ISS was greatest in the early group (P < 0.05). Initial head CT Marshall scores were similar in early and late groups. The slowest progression of brain injury on repeated head CT scans was in the early VTEp group up to 10 days after admission.
Conclusion: Early initiation of prophylactic heparin in severe TBI is not associated with deterioration neurologic exam and may result in less progression of injury on brain imaging. Possible neuroprotective effects of heparin in humans need further investigation.
Keywords: Heparin; VTE prophylaxis; intracranial hemorrhage; traumatic brain injury.
Conflict of interest statement
Figures
References
-
- Faul M, Xu L, Wald MM, Coronado VG. Traumatic Brain Injury in the United States: Emergency Department Visits, Hospitalizations and Deaths 2002-2006. Atlanta. 2010
-
- Helmy A, Vizcaychipi M, Gupta AK. Traumatic brain injury: Intensive care management. Br J Anaesth. 2007;99:32–42. - PubMed
-
- Pascual JL, Georgoff P, Maloney-Wilensky E, Sims C, Sarani B, Stiefel MF, et al. Reduced brain tissue oxygen in traumatic brain injury: Are most commonly used interventions successful.? J Trauma. 2011;70:535–46. - PubMed
-
- Reiff DA, Haricharan RN, Bullington NM, Griffin RL, McGwin G, Jr, Rue LW, 3rd, et al. Traumatic brain injury is associated with the development of deep vein thrombosis independent of pharmacological prophylaxis. J Trauma. 2009;66:1436–40. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials