

Learning curve of sutureless transconjunctival 20-gauge vitrectomy
- PMID: 25114498
- PMCID: PMC4109639
- DOI: 10.2147/OPTH.S61756
Learning curve of sutureless transconjunctival 20-gauge vitrectomy
Abstract
Background: To report the learning curve of transition from 20-gauge (20 G) conventional vitrectomy to a 20 G sutureless vitrectomy technique.
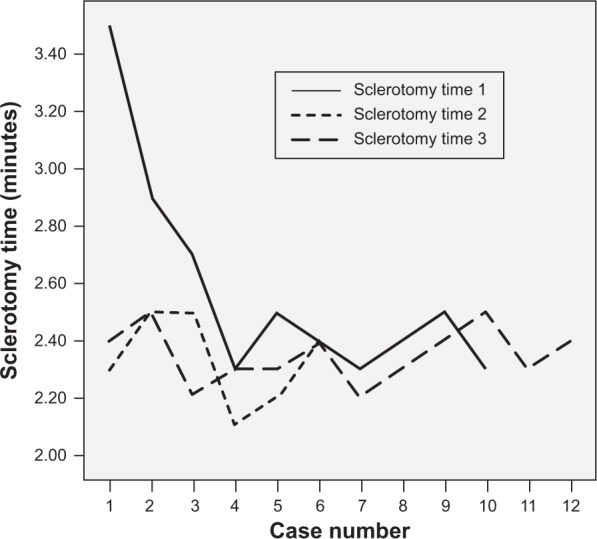
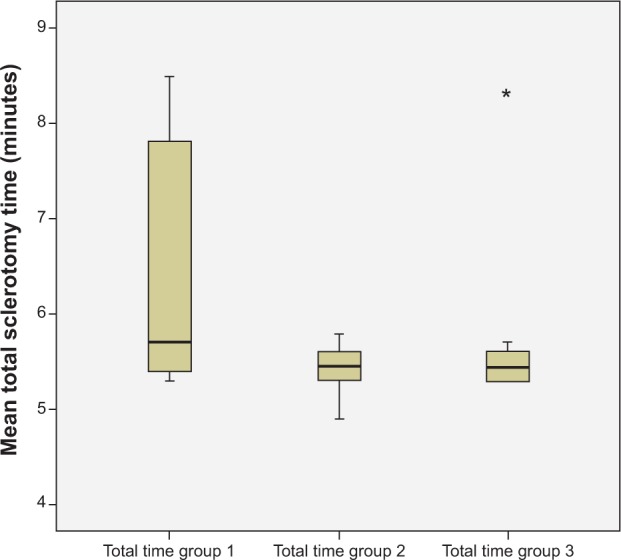
Materials and methods: This is a retrospective descriptive case study of 32 eyes from 32 consecutive patients who underwent sutureless 20 G pars plana vitrectomy. A 20 G microvitreoretinal blade was introduced, beveled transconjunctivally, slowly, parallel with the limbus, creating a conjunctivoscleral tunnel incision. Study participants were divided into three groups, and surgical time, induced astigmatism, and complications were compared.
Results: Of 32 consecutive patients, there was no significant difference in induced astigmatism or maneuvering between the early learning curve and other groups. The true learning curve was the first three patients. There were three cases where suturing the sclerotomy was necessary: one port in each case, three of 32 cases (9.3%), or three of 96 ports (2.9%).
Conclusion: There were no significant difficulties in surgical maneuvers while performing 20 g sutureless vitrectomy.
Keywords: 20 G; learning curve; sutureless; vitrectomy.
Figures
References
-
- Machemer R, Buettner H, Norton EW, Parel JM. Vitrectomy: a pars plana approach. Trans Am Acad Ophthalmol Otolaryngol. 1971;75:813–820. - PubMed
-
- Kadonosono K, Yamakawa T, Uchio E, Yanagi Y, Tamaki Y, Araie M. Comparison of visual function after epiretinal membrane removal by 20-gauge and 25-gauge vitrectomy. Am J Ophthalmol. 2006;142:513–515. - PubMed
-
- Yanyali A, Celik E, Horozoglu F, Oner S, Nohutcu AF. 25-gauge transconjunctival sutureless pars plana vitrectomy. Eur J Ophthalmol. 2006;16:141–147. - PubMed
-
- Yanyali A, Celik E, Horozoglu F, Nohutcu AF. Corneal topographic changes after transconjunctival (25-gauge) sutureless vitrectomy. Am J Ophthalmol. 2005;140:939–941. - PubMed
-
- Fujii GY, De Juan E, Jr, Humayun MS, et al. A new 25-gauge instrument system for transconjunctival sutureless vitrectomy surgery. Ophthalmology. 2002;109:1807–1812. discussion 1813. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
