

Pulmonary function impairment in patients with combined pulmonary fibrosis and emphysema with and without airflow obstruction
- PMID: 25114520
- PMCID: PMC4122579
- DOI: 10.2147/COPD.S65621
Pulmonary function impairment in patients with combined pulmonary fibrosis and emphysema with and without airflow obstruction
Abstract
Background: The syndrome of combined pulmonary fibrosis and emphysema (CPFE) is a recently described entity associating upper-lobe emphysema and lower-lobe fibrosis. We sought to evaluate differences in pulmonary function between CPFE patients with and without airflow obstruction.
Subjects and methods: Thirty-one CPFE patients were divided into two groups according to the presence or absence of irreversible airflow obstruction based on spirometry (forced expiratory volume in 1 second/forced vital capacity <70% following inhalation of a β2-agonist) as follows: CPFE patients with airflow obstruction (CPFE OB(+) group, n=11), and CPFE patients without airflow obstruction (CPFE OB(-) group, n=20). Pulmonary function, including respiratory impedance evaluated using impulse oscillometry and dynamic hyperinflation following metronome-paced incremental hyperventilation, was retrospectively analyzed in comparison with that observed in 49 chronic obstructive pulmonary disease (COPD) patients (n=49).
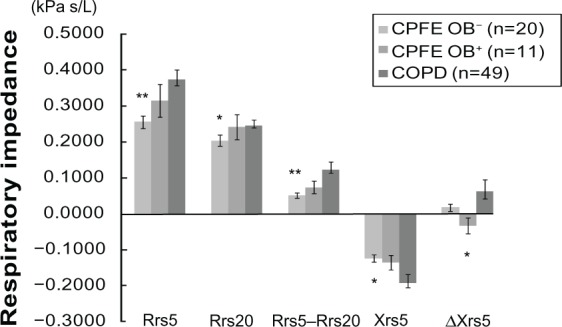
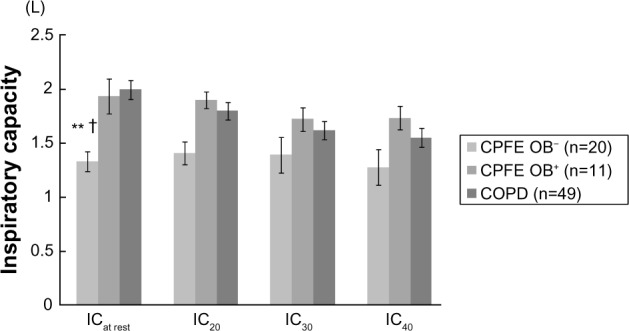
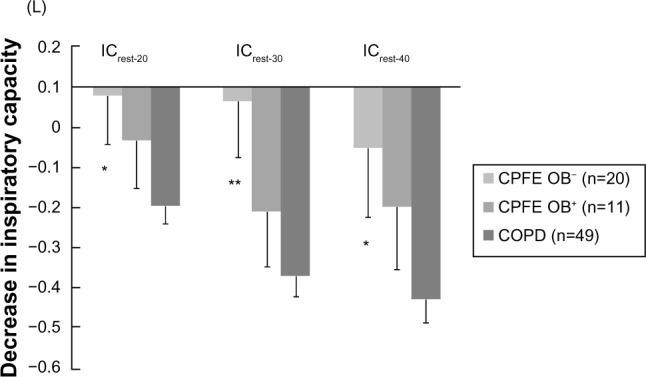
Results: In imaging findings, low-attenuation-area scores on chest high-resolution computed tomography, representing the degree of emphysema, were significantly lower in the CPFE OB(-) group than in the CPFE OB(+) and COPD groups. In contrast, the severity of pulmonary fibrosis was greater in the CPFE OB(-) group than in the CPFE OB(+) group. In pulmonary function, lung hyperinflation was not apparent in the CPFE OB(-) group. Impairment of diffusion capacity was severe in both the CPFE OB(-) and CPFE OB(+) groups. Impulse oscillometry showed that respiratory resistance was not apparent in the CPFE OB(-) group compared with the COPD group, and that easy collapsibility of small airways during expiration of tidal breath was not apparent in the CPFE OB(+) group compared with the COPD group. Dynamic hyperinflation following metronome-paced incremental hyperventilation was significantly greater in the COPD group than in the CPFE OB(-) group, and also tended to be greater in the CPFE OB(+) group than in the CPFE OB(-) group.
Conclusion: The mechanisms underlying impairment of physiological function may differ among CPFE OB(+) patients, CPFE OB(-) patients, and COPD patients. CPFE is a heterogeneous disease, and may have distinct phenotypes physiologically and radiologically.
Keywords: COPD; CPFE; dynamic hyperinflation; respiratory impedance.
Figures
Similar articles
-
Relationship between quantitative CT metrics and pulmonary function in combined pulmonary fibrosis and emphysema.Lung. 2013 Dec;191(6):585-91. doi: 10.1007/s00408-013-9513-1. Epub 2013 Oct 2. Lung. 2013. PMID: 24085320
-
Respiratory mechanics measured by forced oscillation technique in combined pulmonary fibrosis and emphysema.Respir Physiol Neurobiol. 2013 Jan 15;185(2):235-40. doi: 10.1016/j.resp.2012.10.009. Epub 2012 Oct 29. Respir Physiol Neurobiol. 2013. PMID: 23117106
-
Comparison of pulmonary function in patients with COPD, asthma-COPD overlap syndrome, and asthma with airflow limitation.Int J Chron Obstruct Pulmon Dis. 2016 May 9;11:991-7. doi: 10.2147/COPD.S105988. eCollection 2016. Int J Chron Obstruct Pulmon Dis. 2016. PMID: 27274220 Free PMC article.
-
Pulmonary hypertension in chronic lung diseases.J Am Coll Cardiol. 2013 Dec 24;62(25 Suppl):D109-16. doi: 10.1016/j.jacc.2013.10.036. J Am Coll Cardiol. 2013. PMID: 24355635 Review.
-
Combined Pulmonary Fibrosis and Emphysema: Pulmonary Function Testing and a Pathophysiology Perspective.Medicina (Kaunas). 2019 Sep 10;55(9):580. doi: 10.3390/medicina55090580. Medicina (Kaunas). 2019. PMID: 31509942 Free PMC article. Review.
Cited by
-
Chest CT scan for the screening of air anomalies at risk of pulmonary barotrauma for the initial medical assessment of fitness to dive in a military population.Front Physiol. 2022 Oct 7;13:1005698. doi: 10.3389/fphys.2022.1005698. eCollection 2022. Front Physiol. 2022. PMID: 36277200 Free PMC article.
-
Objective quantitative multidetector computed tomography assessments in patients with combined pulmonary fibrosis with emphysema: Relationship with pulmonary function and clinical events.PLoS One. 2020 Sep 17;15(9):e0239066. doi: 10.1371/journal.pone.0239066. eCollection 2020. PLoS One. 2020. PMID: 32941486 Free PMC article.
-
Combined Pulmonary Fibrosis and Emphysema Syndrome: What is the Role of Airflow Limitation?Open Respir Arch. 2023 Feb 1;5(1):100233. doi: 10.1016/j.opresp.2023.100233. eCollection 2023 Jan-Mar. Open Respir Arch. 2023. PMID: 37497242 Free PMC article. No abstract available.
-
The Evaluation of Interstitial Abnormalities in Group B of the 2011 Global Initiative for Chronic Obstructive Lung Disease (GOLD) Classification of Chronic Obstructive Pulmonary Disease (COPD).Intern Med. 2017 Oct 15;56(20):2711-2717. doi: 10.2169/internalmedicine.8406-16. Epub 2017 Sep 15. Intern Med. 2017. PMID: 28924113 Free PMC article.
-
Combined pulmonary fibrosis and emphysema (CPFE): an entity different from emphysema or pulmonary fibrosis alone.J Thorac Dis. 2015 Apr;7(4):767-79. doi: 10.3978/j.issn.2072-1439.2015.04.17. J Thorac Dis. 2015. PMID: 25973246 Free PMC article. Review.
References
-
- Cottin V, Nunes H, Brillet PY, et al. Combined pulmonary fibrosis and emphysema: a distinct underrecognised entity. Eur Respir J. 2005;26:586–593. - PubMed
-
- Jankowich MD, Polsky M, Klein M, Rounds S. Heterogeneity in combined pulmonary fibrosis and emphysema. Respiration. 2008;75:411–417. - PubMed
-
- Kitaguchi Y, Fujimoto K, Hanaoka M, Kawakami S, Honda T, Kubo K. Clinical characteristics of combined pulmonary fibrosis and emphysema. Respirology. 2010;15:265–271. - PubMed
-
- Grubstein A, Bendayan D, Schactman I, Cohen M, Shitrit D, Kramer MR. Concomitant upper-lobe bullous emphysema, lower-lobe interstitial fibrosis and pulmonary hypertension in heavy smokers: report of eight cases and review of the literature. Respir Med. 2005;99:948–954. - PubMed
-
- Mura M, Zompatori M, Pacilli AM, Fasano L, Schiavina M, Fabbri M. The presence of emphysema further impairs physiologic function in patients with idiopathic pulmonary fibrosis. Respir Care. 2006;51:257–265. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
