

Breast reconstruction following prophylactic or therapeutic mastectomy for breast cancer: Recommendations from an evidence-based provincial guideline
- PMID: 25114623
- PMCID: PMC4116309
Breast reconstruction following prophylactic or therapeutic mastectomy for breast cancer: Recommendations from an evidence-based provincial guideline
Abstract
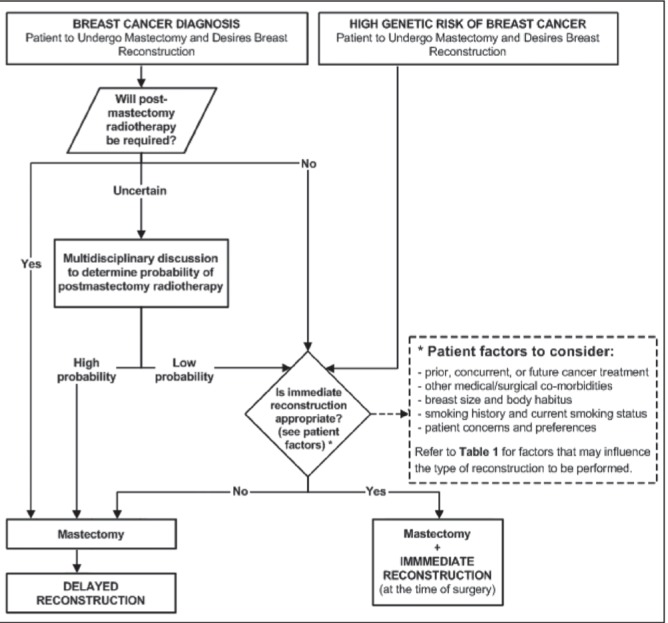
The side effects of mastectomy can be significant. Breast reconstruction may alleviate some distress; however, there are currently no provincial recommendations regarding the integration of reconstruction with breast cancer therapy. The purpose of the present article is to provide evidence-based strategies for the management of patients who are candidates for reconstruction. A systematic review of meta-analyses, guidelines, clinical trials and comparative studies published between 1980 and 2013 was conducted using the PubMed and EMBASE databases. Reference lists of publications were manually searched for additional literature. The National Guidelines Clearinghouse and SAGE directory, as well as guideline developers' websites, were also searched. Recommendations were developed based on the available evidence. Reconstruction consultation should be made available for patients undergoing mastectomy. Tumour characteristics, cancer therapy, patient comorbidities, body habitus and smoking history may affect reconstruction outcomes. Although immediate reconstruction should be considered whenever possible, delayed reconstruction is acceptable when immediate is not available or appropriate. The integration of reconstruction and postmastectomy radiotherapy should be addressed in a multidisciplinary setting. The decision as to which type of procedure to perform (autologous or alloplastic with or without acellular dermal matrices) should be left to the discretion of the surgeons and the patient after providing counselling. Skin-sparing mastectomy is safe and appropriate. Nipple-sparing is generally not recommended for patients with malignancy, but could be considered for carefully selected patients. Immediate reconstruction requires resources to coordinate operating room time between the general and plastic surgeons, to provide supplies including acellular dermal matrices, and to develop the infrastructure needed to facilitate multidisciplinary discussions.
La mastectomie peut avoir des effets secondaires importants. La reconstruction mammaire peut soulager une certaine détresse, mais il n’existe pas de recommandations provinciales sur l’intégration de la reconstruction au traitement du cancer du sein. Le présent article vise à fournir des stratégies fondées sur des données probantes sur la prise en charge des patientes candidates à la reconstruction. Les auteurs ont effectué une analyse systématique des méta-analyses, des lignes directrices, des essais cliniques et des études comparatives publiées entre 1980 et 2013 obtenus dans les bases de données PubMed et EMBASE. Ils ont fait des recherches manuelles dans les listes de référence des publications pour trouver d’autres articles. Ils ont également fouillé le National Guidelines Clearinghouse et le répertoire SAGE, de même que les sites Web des développeurs de lignes directrices. Ils ont fait des recommandations d’après les données probantes disponibles. Les patientes qui subissent une mastectomie devraient profiter d’une consultation sur la reconstruction. Les caractéristiques des tumeurs, le traitement du cancer, les comorbidités des patients, le phénotype corporel et les antécédents de tabagisme peuvent nuire aux résultats de la reconstruction. Même s’il faut envisager une reconstruction immédiate dans la mesure du possible, il est acceptable de la reporter lorsque ce n’est pas possible ou envisageable. Une équipe multidisciplinaire doit discuter de l’intégration de la reconstruction et de la radiothérapie après la mastectomie. Il faut laisser le chirurgien et le patient décider du type d’intervention à privilégier (autologue ou alloplastique, accompagnée ou non de matrices dermiques acellulaires) après avoir offert des conseils thérapeutiques. La mastectomie qui épargne la peau est sécuritaire et pertinente. Il n’est généralement pas recommandé d’épargner le mamelon chez les patientes ayant une tumeur maligne, mais on peut l’envisager auprès de patientes soigneusement sélectionnées. Il faut des ressources pour effectuer une reconstruction immédiate afin de coordonner le temps opératoire entre les plasticiens généraux et plastiques, de fournir le matériel, y compris les matrices dermiques acellulaires, et de prévoir l’infrastructure nécessaire pour faciliter les discussions multidisciplinaires.
Keywords: Breast cancer; Breast reconstruction; Guideline; Mastectomy.
Figures
Similar articles
-
Bilateral prophylactic mastectomy in BRCA mutation carriers: what surgeons need to know.Ann Ital Chir. 2019;90:1-2. Ann Ital Chir. 2019. PMID: 30872561
-
Breast reconstruction after therapeutic or prophylactic mastectomy for breast cancer: A comparison of guideline recommendations.Eur J Surg Oncol. 2020 Jun;46(6):1046-1051. doi: 10.1016/j.ejso.2020.01.024. Epub 2020 Jan 18. Eur J Surg Oncol. 2020. PMID: 32057564 Review.
-
Staged Suprapectoral Expander/Implant Reconstruction without Acellular Dermal Matrix following Nipple-Sparing Mastectomy.Plast Reconstr Surg. 2017 Jan;139(1):30-39. doi: 10.1097/PRS.0000000000002845. Plast Reconstr Surg. 2017. PMID: 28027223 Clinical Trial.
-
Prepectoral Direct-to-Implant Breast Reconstruction without Placement of Acellular Dermal Matrix or Mesh after Nipple-Sparing Mastectomy.Plast Reconstr Surg. 2022 Nov 1;150(5):973-983. doi: 10.1097/PRS.0000000000009618. Epub 2022 Aug 19. Plast Reconstr Surg. 2022. PMID: 35994351
-
Defining a place for nipple sparing mastectomy in modern breast care: an evidence based review.Breast J. 2013 Nov-Dec;19(6):571-81. doi: 10.1111/j.1524-4741.2011.01220.x. Epub 2012 Jan 29. Breast J. 2013. PMID: 22284266 Review.
Cited by
-
Jumping Breast Phenomenon Following Subcutaneous Mastectomy: First Description and Grading of a Well-Known Breast Deformity.Breast Care (Basel). 2018 Oct;13(5):354-358. doi: 10.1159/000489939. Epub 2018 Aug 3. Breast Care (Basel). 2018. PMID: 30498421 Free PMC article.
-
Patient-Reported Satisfaction Following Radiation of Implant-Based Breast Reconstruction.Plast Surg (Oakv). 2019 May;27(2):147-155. doi: 10.1177/2292550319826090. Epub 2019 Mar 13. Plast Surg (Oakv). 2019. PMID: 31106173 Free PMC article.
-
Impact of different type of cancer treatment on the effectiveness of breast reconstruction.Gland Surg. 2016 Aug;5(4):444-9. doi: 10.21037/gs.2016.05.06. Gland Surg. 2016. PMID: 27562472 Free PMC article.
-
Impact of Immediate and Delayed Breast Reconstruction on Quality of Life of Breast Cancer Patients.Int J Environ Res Public Health. 2022 Jul 13;19(14):8546. doi: 10.3390/ijerph19148546. Int J Environ Res Public Health. 2022. PMID: 35886396 Free PMC article.
-
Breast Implant Rupture Surveillance Practices among Plastic Surgeons in Publicly Funded Healthcare Systems.Aesthetic Plast Surg. 2025 Feb;49(3):741-748. doi: 10.1007/s00266-024-04345-y. Epub 2024 Sep 12. Aesthetic Plast Surg. 2025. PMID: 39266683
References
-
- National Comprehensive Cancer Network Breast Cancer Clinical Practice Guidelines in Oncology Version 1.2012. < www.nccn.org> (Accessed August 10, 2012). - PubMed
-
- Cancer Care Ontario Program in Evidence-Based Care. Surgical Management of Early-Stage Invasive Breast Cancer. Practice Guideline Report #1-1 Version 2.2003 (updated 2010) < www.cancercare.on.ca/common/pages/UserFile.aspx?fileId=34102> (Accessed August 10, 2012).
-
- Canadian Partnership Against Cancer and Canadian Institute for Health Information Breast Cancer Surgery in Canada, 2007–2008 to 2009–2010. < http://publications.gc.ca/collections/collection_2012/icis-cihi/H115-61-...> (Accessed December 31, 2012).
-
- CancerControl Alberta Treatment Guidelines: Risk Reduction and Surveillance Strategies for Individuals at High Genetic Risk for Breast and Ovarian Cancer. The Provincial Breast Tumour Team and the Guideline Utilization Resource Unit. < www.albertahealthservices.ca/hp/if-hp-cancer-guide-br011-hereditary-risk...> (Accessed August 10, 2012).
-
- Horsman D, Wilson BJ, Avard D, et al. National Hereditary Cancer Task Force Clinical management recommendations for surveillance and risk reduction strategies for hereditary breast and ovarian cancer among individuals carrying a deleterious BRCA1 or BRCA2 mutation. J Obstet Gynaecol Can. 2007;29:45–60. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources