

Clinical presentation and magnetic resonance findings in sellar tuberculomas
- PMID: 25114688
- PMCID: PMC4119910
- DOI: 10.1155/2014/961913
Clinical presentation and magnetic resonance findings in sellar tuberculomas
Abstract
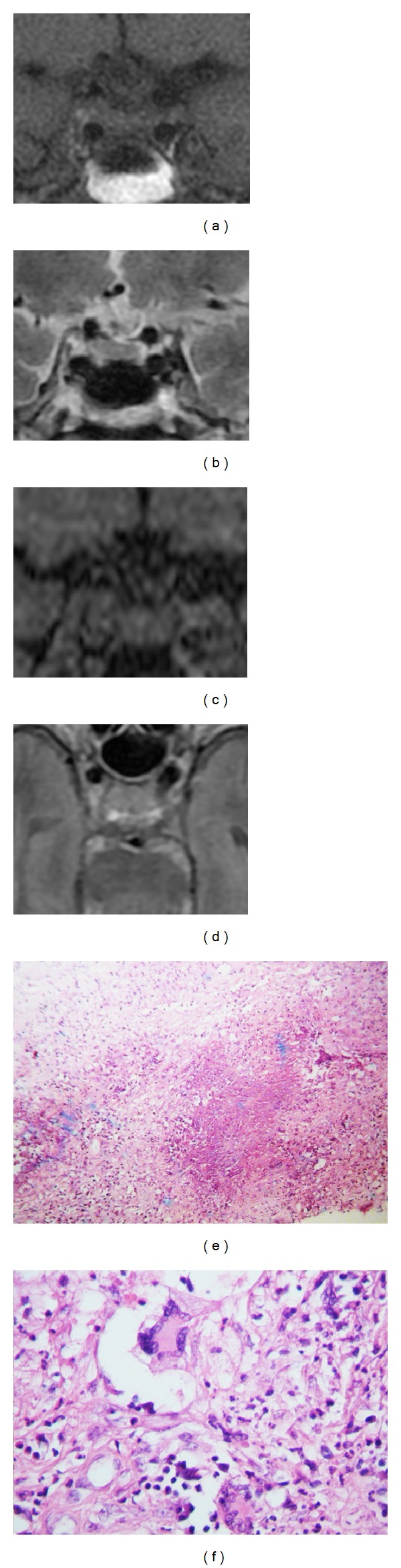
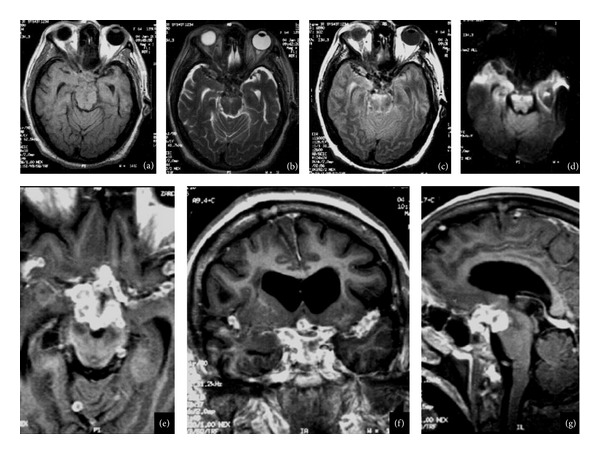
Background and Importance. Sellar tuberculomas are extremely rare lesions with nonspecific clinical manifestations. The tuberculous infection of the pituitary gland and sellar region is characterized by the presence of an acute or chronic inflammatory reaction and may occur in the absence of systemic tuberculosis. The diagnosis is difficult prior to the surgery. An adequate diagnostic and antituberculous drugs usually result in a good outcome. Clinical Presentation. We report four cases of sellar tuberculoma, 3/1 female/male, age range: 50-57 years. All patients had visual disturbances and low levels of cortisol. Conclusion. The clinical diagnosis of sellar tuberculoma is a challenge and should be suspected when a sellar lesion shows abnormal enhancement pattern and stalk involvement, and absence of signal suppression in FLAIR.
Figures


References
-
- von Groote-Bidlingmaier F, Diacon AH. Medical treatment of tuberculosis-update 2011. Therapeutische Umschau Revue Therapeutique . 2011;68(7):395–401. - PubMed
-
- Sunil K, Menon R, Goel N, et al. Pituitary tuberculosis. Journal of Association of Physicians of India. 2007;55:453–456. - PubMed
-
- Arunkumar MJ, Rajshekhar V. Intrasellar tuberculoma presenting as pituitary apoplexy. Neurology India. 2001;49(4):407–410. - PubMed
-
- Garlan HG, Armitage G. Intracranial tuberculoma. The Journal of Pathology and Bacteriology. 1933;37(3):461–471.
-
- Coleman CC, Meredith JM. Diffuse tuberculosis of the pituitary gland simulating tumor, with postoperative recovery. Archives of Neurology and Psychiatry. 1940;44:1076–1085.
LinkOut - more resources
Full Text Sources
Other Literature Sources
