

Peri-procedural interrupted oral anticoagulation for atrial fibrillation ablation: comparison of aspirin, warfarin, dabigatran, and rivaroxaban
- PMID: 25115168
- PMCID: PMC4178475
- DOI: 10.1093/europace/euu196
Peri-procedural interrupted oral anticoagulation for atrial fibrillation ablation: comparison of aspirin, warfarin, dabigatran, and rivaroxaban
Abstract
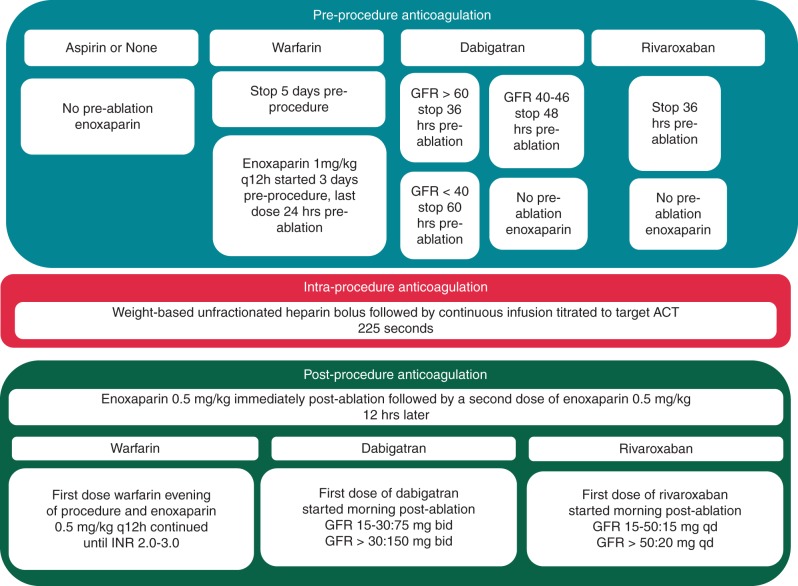
Aims: Atrial fibrillation ablation requires peri-procedural oral anticoagulation (OAC) to prevent thromboembolic events. There are several options for OAC. We evaluate peri-procedural AF ablation complications using a variety of peri-procedural OACs.
Methods and results: We examined peri-procedural OAC and groin, bleeding, and thromboembolic complications for 2334 consecutive AF ablations using open irrigated-tip radiofrequency (RF) catheters. Pre-ablation OAC was warfarin in 1113 (47.7%), dabigatran 426 (18.3%), rivaroxaban 187 (8.0%), aspirin 472 (20.2%), and none 136 (5.8%). Oral anticoagulation was always interrupted and intraprocedural anticoagulation was unfractionated heparin (activated clotting time, ACT = 237 ± 26 s). Pre- and post-OAC drugs were the same for 1591 (68.2%) and were different for 743 (31.8%). Following ablation, 693 (29.7%) were treated with dabigatran and 291 (12.5%) were treated with rivaroxaban. There were no problems changing from one OAC pre-ablation to another post-ablation. Complications included 12 (0.51%) pericardial tamponades [no differences for dabigatran (P = 0.457) or rivaroxaban (P = 0.163) compared with warfarin], 12 (0.51%) groin complications [no differences for rivaroxaban (P = 0.709) and fewer for dabigatran (P = 0.041) compared with warfarin]. Only 5 of 2334 (0.21%) required blood transfusions. There were two strokes (0.086%) and no transient ischaemic attacks (TIAs) in the first 48 h post-ablation. Three additional strokes (0.13%), and two TIAs (0.086%) occurred from 48 h to 30 days. Only one stroke had a residual deficit. Compared with warfarin, the neurologic event rate was not different for dabigatran (P = 0.684) or rivaroxaban (P = 0.612).
Conclusion: Using interrupted OAC, low target intraprocedural ACT, and irrigated-tip RF, the rate of peri-procedural groin, haemorrhagic, and thromboembolic complications was extremely low. There were only minimal differences between OACs. Low-risk patients may remain on aspirin/no OAC pre-ablation. There are no problems changing from one OAC pre-ablation to another post-ablation.
Keywords: Ablation; Anticoagulation; Atrial fibrillation; Dabigatran; Rivaroxaban; Warfarin.
© The Author 2014. Published by Oxford University Press on behalf of the European Society of Cardiology.
Figures
References
-
- Calkins H, Brugada J, Packer DL, Capppato R, Chen S, Crijns H, et al. HRS/EHRA/ECAS expert consensus statement on catheter and surgical ablation of atrial fibrillation: recommendations for personnel, policy, procedures and follow-up. Europace. 2007;9:335–79. - PubMed
-
- Wann LS, Curtis AB, January CT, Ellenbogen KA, Lowe JE, Estes M, et al. 2011 ACCF/AHA/HRS focused update on the management of patients with atrial fibrillation (updating the 2006 guideline): a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. Heart Rhythm. 2011;8:157–76. - PubMed
-
- O'Neill MD, Wright M, Knecht S, Jais P, Hocini M, Takahashi Y, et al. Long-term follow-up of persistent atrial fibrillation ablation using termination as a procedural endpoint. Eur Heart J. 2009;30:1105–12. - PubMed
-
- Winkle RA, Mead RH, Engel G, Patrawala RA. Long term results of atrial fibrillation ablation: the importance of all initial ablation failures undergoing a repeat ablation. Am Heart J. 2011;162:193–200. - PubMed
-
- Hussein AA, Martin DO, Saliba W, Patel D, Karim S, Batal O, et al. Radiofrequency ablation of atrial fibrillation under therapeutic international normalized ratio: a safe and efficacious periprocedural anticoagulation strategy. Heart Rhythm. 2009;6:1425–9. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
