

Implantable collamer lens versus iris-fixed phakic intraocular lens implantation to correct myopia: a meta-analysis
- PMID: 25115906
- PMCID: PMC4130551
- DOI: 10.1371/journal.pone.0104649
Implantable collamer lens versus iris-fixed phakic intraocular lens implantation to correct myopia: a meta-analysis
Abstract
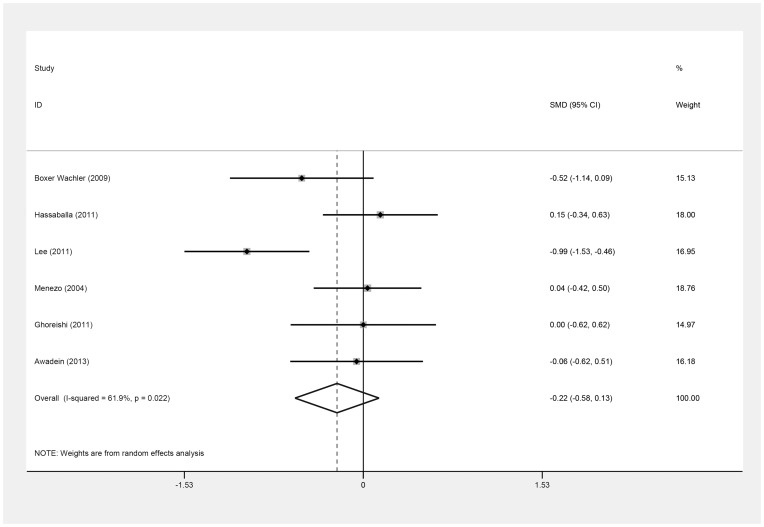
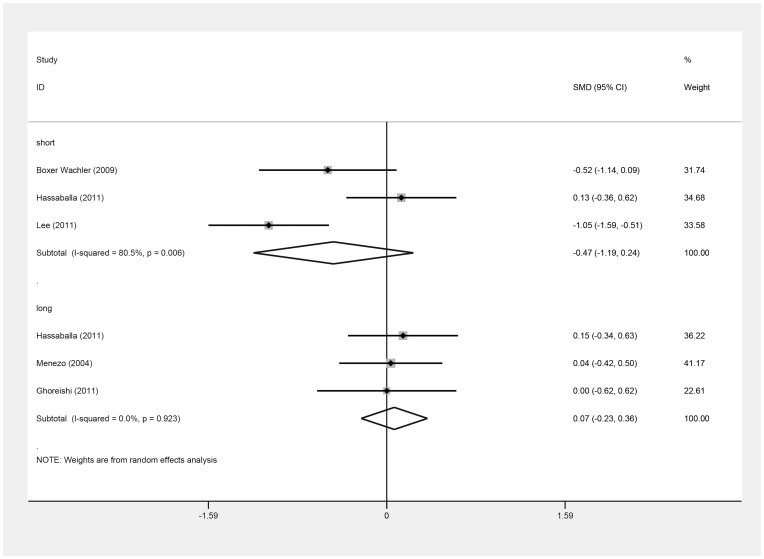
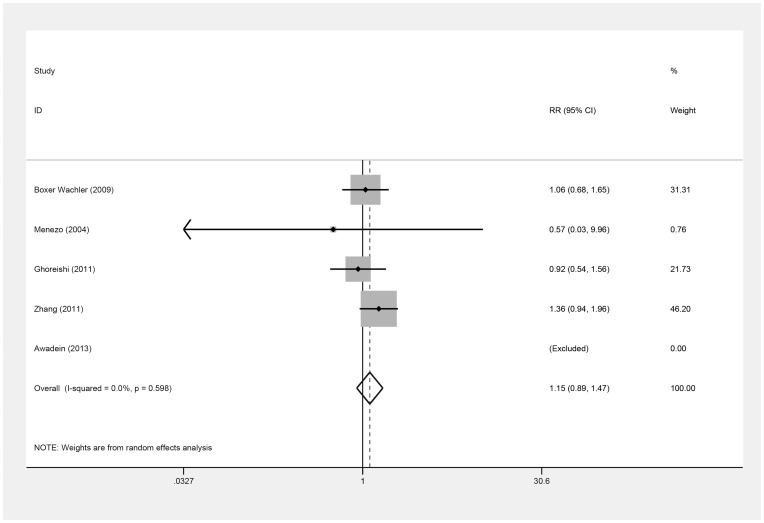
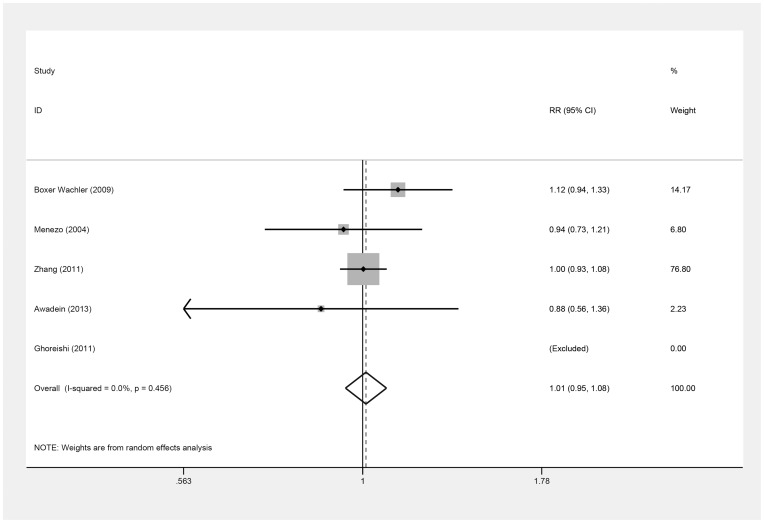
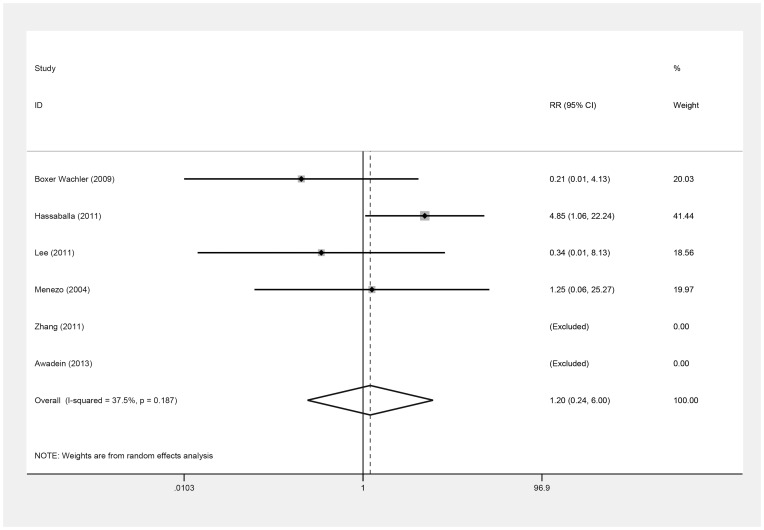
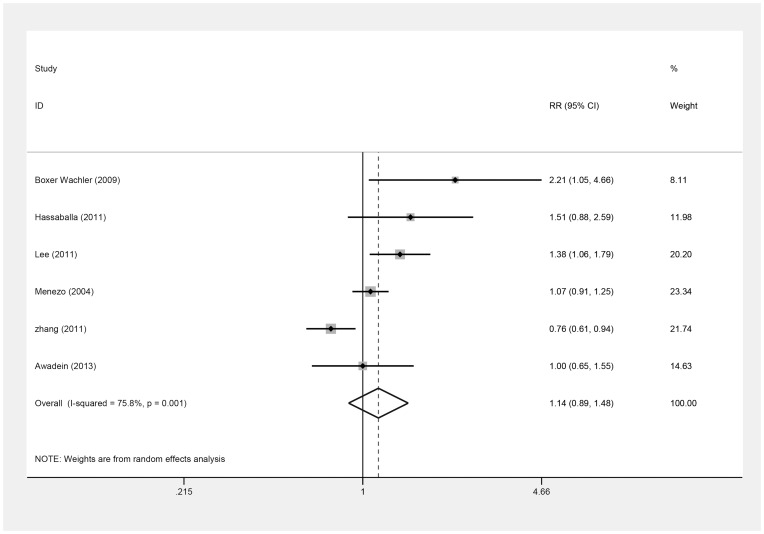
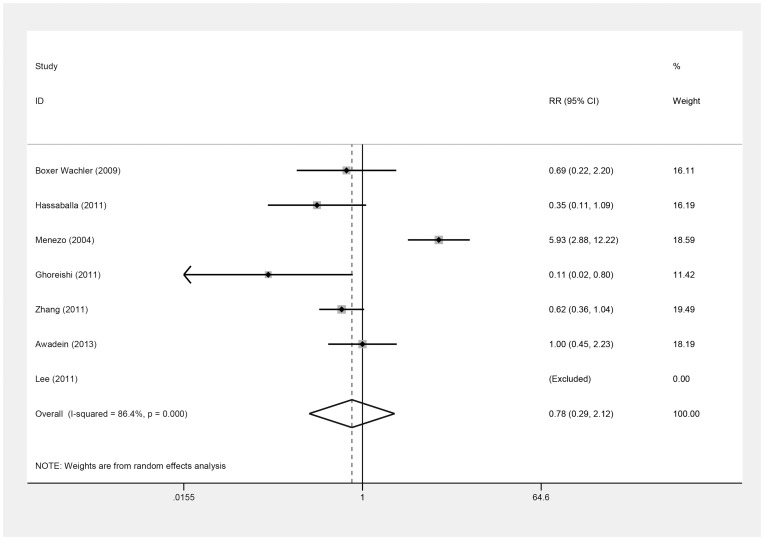
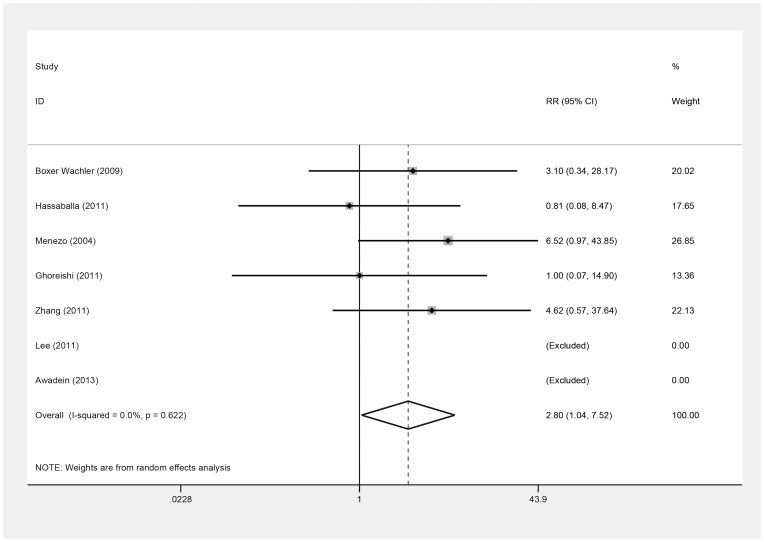
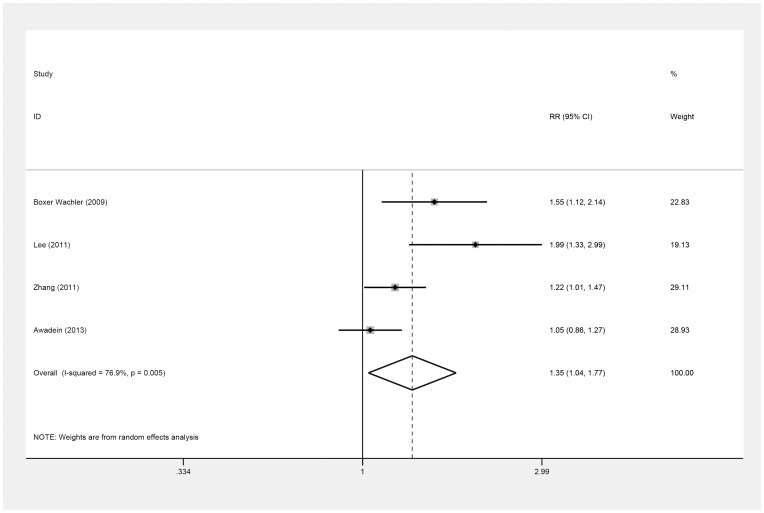
This study is a meta-analysis comparing the efficacy, predictability, and safety of correcting myopia via implantation of two types of phakic intraocular lens (PIOLs): the implantable collamer lens (ICL) and iris-fixed PIOL. The Cochrane library, Pubmed, and EMBASE were searched. Study selection, data exclusion, and quality assessment were performed by two independent observers. The pooled relative risk (RR), pooled standardized mean difference (SMD), and their 95% confidence intervals (CIs) were used to compare lenses. Seven studies, involving 511 eyes, were included. The pooled SMD in postoperative uncorrected distance visual acuity (UDVA) comparing ICLs to iris-fixed PIOLs was -0.22 (95% CI, -0.58 to 0.13; P = .22). The pooled RR values of UDVA of 20/20 or better and of 20/40 or better comparing ICLs to iris-fixed PIOLs were 1.15 (95% CI, 0.89 to 1.47; P = .29) and 1.01 (95% CI, 0.95 to 1.08; P = .75), respectively. The pooled RR of loss of best spectacle-corrected visual acuity (BSCVA) and gain in BSCVA comparing ICLs to iris-fixed PIOLs were 1.20 (95% CI, 0.24 to 6.00; P = .82) and 1.14 (95% CI, 0.89 to 1.48; P = .31), respectively. The pooled RR comparing ICLs to iris-fixed PIOLs was 0.78 (95% CI, 0.29 to 2.12; P = .63) for all reported complications and 2.80 (95% CI, 1.04 to 7.52; P = .04) for severe complications. The pooled RR of achieving a result within ± 0.5 D (diopter) of the intended target comparing ICLs to iris-fixed PIOLs was 1.35 (95% CI, 1.04 to 1.77; P = .03). Overall, there is no significant difference in efficacy between the two types of PIOLs or in safety, except that the ICL is associated with a greater incidence of severe complications, especially anterior subcapsular cataract, primarily in the Version 2 and Version 3 groups. However, ICL has better predictability.
Conflict of interest statement
Figures
Similar articles
-
Comparison of the visual performance of iris-fixated phakic lens and implantable collamer lens to correct high myopia.BMC Ophthalmol. 2021 Jun 2;21(1):244. doi: 10.1186/s12886-021-01995-3. BMC Ophthalmol. 2021. PMID: 34078321 Free PMC article.
-
Phakic intraocular lenses for the treatment of refractive errors: an evidence-based analysis.Ont Health Technol Assess Ser. 2009;9(14):1-120. Epub 2009 Oct 1. Ont Health Technol Assess Ser. 2009. PMID: 23074518 Free PMC article.
-
Phakic intraocular lens implantation for the correction of myopia: a report by the American Academy of Ophthalmology.Ophthalmology. 2009 Nov;116(11):2244-58. doi: 10.1016/j.ophtha.2009.08.018. Ophthalmology. 2009. PMID: 19883852 Review.
-
Five-year clinical outcomes of rigid iris-fixated phakic intraocular lens in northern Chinese.Int Ophthalmol. 2022 Aug;42(8):2551-2561. doi: 10.1007/s10792-022-02303-8. Epub 2022 Apr 5. Int Ophthalmol. 2022. PMID: 35381897
-
Artisan versus Artiflex phakic intraocular lens implantation in the treatment of moderate to high myopia: meta-analysis.BMC Ophthalmol. 2021 Apr 10;21(1):171. doi: 10.1186/s12886-021-01930-6. BMC Ophthalmol. 2021. PMID: 33838655 Free PMC article. Review.
Cited by
-
Computational simulation of aqueous humour dynamics in the presence of a posterior-chamber versus iris-fixed phakic intraocular lens.PLoS One. 2018 Aug 13;13(8):e0202128. doi: 10.1371/journal.pone.0202128. eCollection 2018. PLoS One. 2018. PMID: 30102728 Free PMC article.
-
Refractive outcomes of implantation of an implantable phakic copolymer lens with peripheral holes in the intraocular posterior chamber in moderate to high myopia patients: a single-surgeon series.Clin Ophthalmol. 2019 Sep 23;13:1887-1894. doi: 10.2147/OPTH.S215821. eCollection 2019. Clin Ophthalmol. 2019. PMID: 31576104 Free PMC article.
-
Dynamic Stimulation Aberrometry: Objectively Measured Accommodation and Pupil Dynamics after Phakic Iris-Fixated Intraocular Lens Implantation.Ophthalmol Sci. 2023 Jul 24;4(2):100374. doi: 10.1016/j.xops.2023.100374. eCollection 2024 Mar-Apr. Ophthalmol Sci. 2023. PMID: 37868795 Free PMC article.
-
A critical evaluation of longitudinal changes of astigmatism following implantation of toric implantable collamer lens (TICL): a comparison between treated and untreated cases over 4 years.Graefes Arch Clin Exp Ophthalmol. 2022 Apr;260(4):1377-1386. doi: 10.1007/s00417-021-05449-w. Epub 2021 Oct 16. Graefes Arch Clin Exp Ophthalmol. 2022. PMID: 34655333
-
Comparison of the visual performance of iris-fixated phakic lens and implantable collamer lens to correct high myopia.BMC Ophthalmol. 2021 Jun 2;21(1):244. doi: 10.1186/s12886-021-01995-3. BMC Ophthalmol. 2021. PMID: 34078321 Free PMC article.
References
-
- Alio JL, Ortiz D, Muftuoglu O, Garcia MJ (2009) Ten years after photorefractive keratectomy (PRK) and laser in situ keratomileusis (LASIK) for moderate to high myopia (control-matched study). Br J Ophthalmol 93: 1313–1318. - PubMed
-
- Seiler T, Wollensak J (1991) Myopic photorefractive keratectomy with the excimer laser. One-year follow-up. Ophthalmology 98: 1156–1163. - PubMed
-
- American Academy of Ophthalmology (1999) Excimer laser photorefractive keratectomy (PRK) for myopia and astigmatism. Ophthalmology 106: 422–437. - PubMed
-
- Schallhorn SC, Farjo AA, Huang D, Boxer Wachler BS, Trattler WB, et al. (2008) Wavefront-guided LASIK for the correction of primary myopia and astigmatism a report by the American Academy of Ophthalmology. Ophthalmology 115: 1249–1261. - PubMed
-
- Sugar A, Rapuano CJ, Culbertson WW, Huang D, Varley GA, et al. (2002) Laser in situ keratomileusis for myopia and astigmatism: safety and efficacy: a report by the American Academy of Ophthalmology. Ophthalmology 109: 175–187. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
