

Quality of dying in the ICU: is it worse for patients admitted from the hospital ward compared to those admitted from the emergency department?
- PMID: 25116294
- PMCID: PMC4350659
- DOI: 10.1007/s00134-014-3425-2
Quality of dying in the ICU: is it worse for patients admitted from the hospital ward compared to those admitted from the emergency department?
Abstract
Objective: Although most intensive care unit (ICU) admissions originate in the emergency department (ED), a substantial number of admissions arrive from hospital wards. Patients transferred from the hospital ward often share clinical characteristics with those admitted from the ED, but family expectations may differ. An understanding of the impact of ICU admission source on family perceptions of end-of-life care may help improve patient and family outcomes by identifying those at risk for poor outcomes.
Design and setting: This was a cohort study of patients with chronic illness and acute respiratory failure requiring mechanical ventilation who died after admission to an ICU in any of the 14 participating hospitals in the Seattle-Tacoma area between 2003 and 2008 (n = 1,500).
Measurements: Using regression models adjusted for hospital site and patient-, nurse- and family-level characteristics, we examined associations between ICU admission source (hospital ward vs. ED) and (1) family ratings of satisfaction with ICU care; (2) family and nurse ratings of quality of dying; (3) chart-based indicators of palliative care.
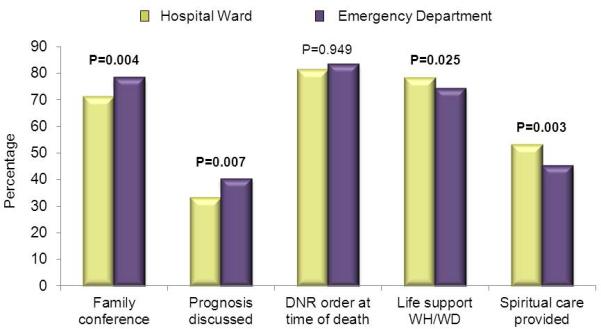
Main results: Admission from the hospital ward was associated with lower family ratings of quality of dying [β -0.90, 95% confidence interval (CI) -1.54, -0.26, p = 0.006] and satisfaction (total score β -3.97, 95% CI -7.89, -0.05, p = 0.047; satisfaction with care domain score β -5.40, 95% CI -9.44, -1.36, p = 0.009). Nurses did not report differences in quality of dying. Patients from hospital wards were less likely to have family conferences [odds ratio (OR) 0.68, 95% CI 0.52, 0.88, p = 0.004] or discussion of prognosis in the first 72 h after ICU admission (OR 0.72, 95% CI 0.56, 0.91, p = 0.007) but were more likely to receive spiritual care (OR 1.48, 95% CI 1.14, 1.93, p = 0.003) or have life support withdrawn (OR 1.38, 95% CI 1.04, 1.82, p = 0.025).
Conclusion: Admission from the hospital ward is associated with family perceptions of a lower quality of dying and less satisfaction with ICU care. Differences in receipt of palliative care suggest that family of patients from the hospital ward receive less communication. Nurse ratings of quality of dying did not significantly differ by ICU admission source, suggesting dissimilarities between family and nurse perspectives. This study identifies a patient population at risk for poor quality palliative and end-of-life care. Future studies are needed to identify interventions to improve care for patients who deteriorate on the wards following hospital admission.
Figures
Comment in
-
Tell me where the patient comes from.Intensive Care Med. 2014 Nov;40(11):1775-7. doi: 10.1007/s00134-014-3462-x. Epub 2014 Sep 3. Intensive Care Med. 2014. PMID: 25183572 No abstract available.
-
Quality of dying in the intensive care unit: it's a matter of time.Intensive Care Med. 2014 Nov;40(11):1792. doi: 10.1007/s00134-014-3499-x. Epub 2014 Oct 7. Intensive Care Med. 2014. PMID: 25288209 No abstract available.
-
Quality of dying in the ICU: understanding ways to make it better.Intensive Care Med. 2014 Nov;40(11):1793. doi: 10.1007/s00134-014-3512-4. Epub 2014 Oct 7. Intensive Care Med. 2014. PMID: 25288214 No abstract available.
References
-
- Angus DC, Shorr AF, White A, Dremsizov TT, Schmitz RJ, Kelley MA. Critical care delivery in the United States: distribution of services and compliance with Leapfrog recommendations. Critical care medicine. 2006;34:1016–1024. - PubMed
-
- Groeger JS, Guntupalli KK, Strosberg M, Halpern N, Raphaely RC, Cerra F, Kaye W. Descriptive analysis of critical care units in the United States: patient characteristics and intensive care unit utilization. Critical care medicine. 1993;21:279–291. - PubMed
-
- Hillman KM, Bristow PJ, Chey T, Daffurn K, Jacques T, Norman SL, Bishop GF, Simmons G. Duration of life-threatening antecedents prior to intensive care admission. Intensive care medicine. 2002;28:1629–1634. - PubMed
-
- Delgado MK, Liu V, Pines JM, Kipnis P, Gardner MN, Escobar GJ. Risk factors for unplanned transfer to intensive care within 24 hours of admission from the emergency department in an integrated healthcare system. Journal of hospital medicine : an official publication of the Society of Hospital Medicine. 2013;8:13–19. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
