

Antibacterial surface treatment for orthopaedic implants
- PMID: 25116685
- PMCID: PMC4159828
- DOI: 10.3390/ijms150813849
Antibacterial surface treatment for orthopaedic implants
Abstract
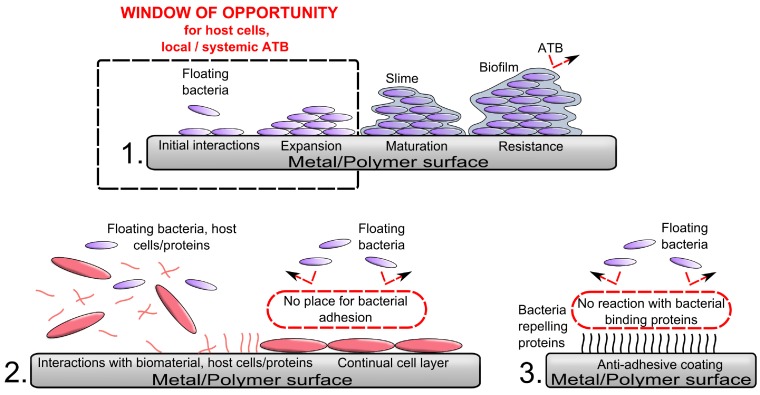
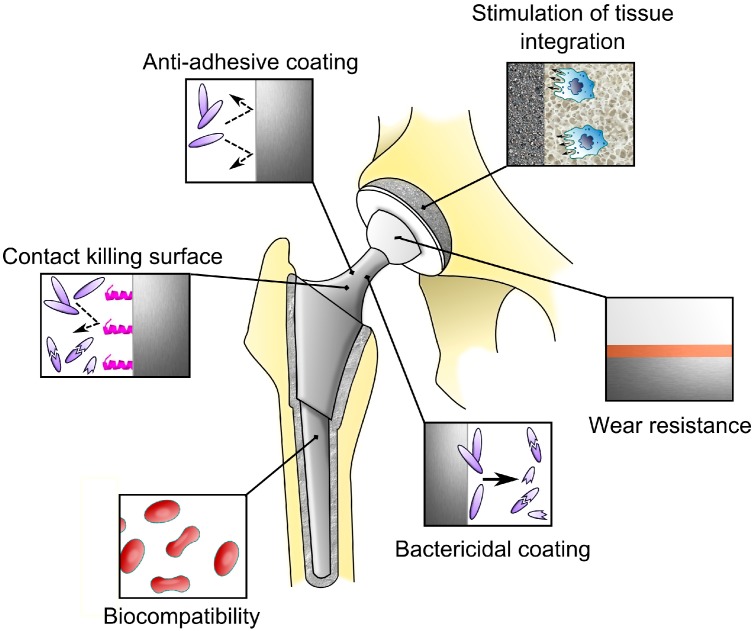
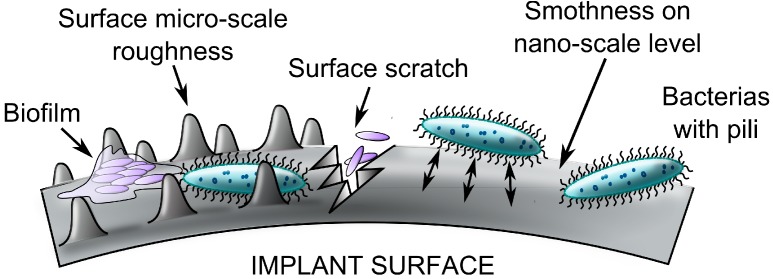
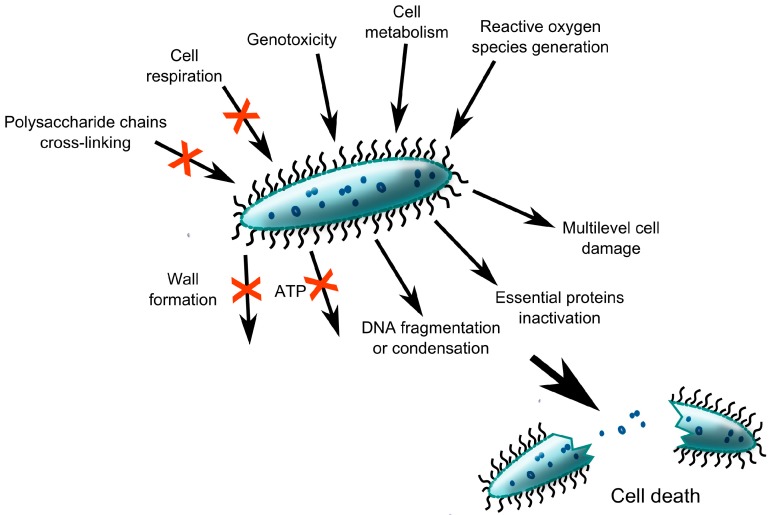
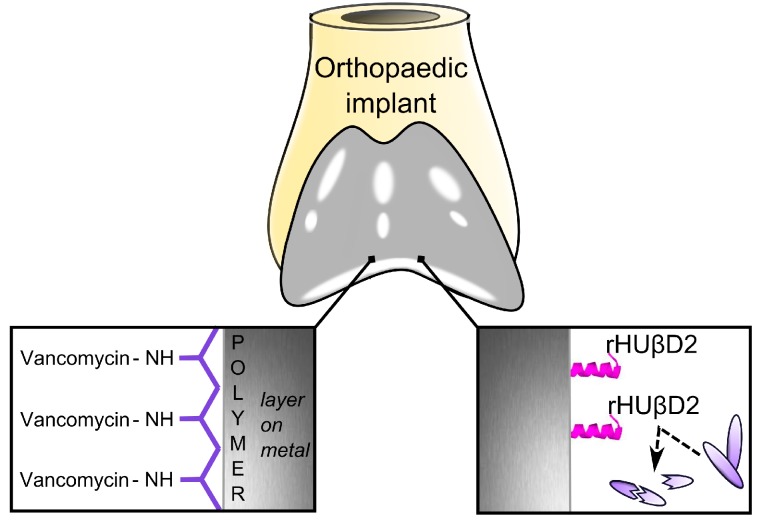
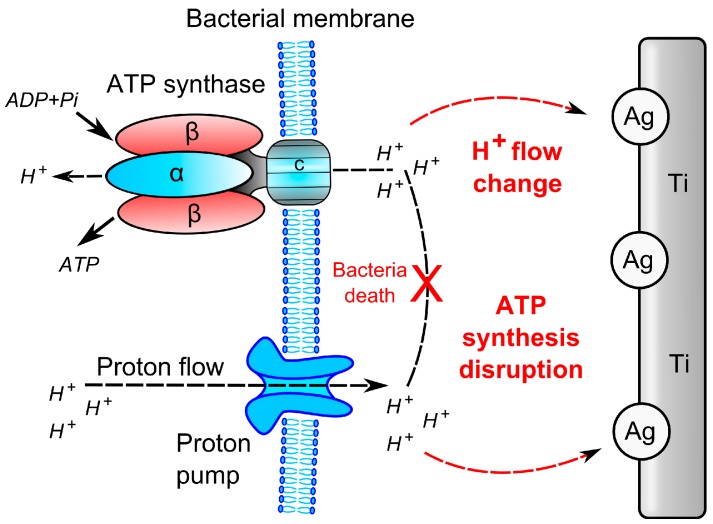
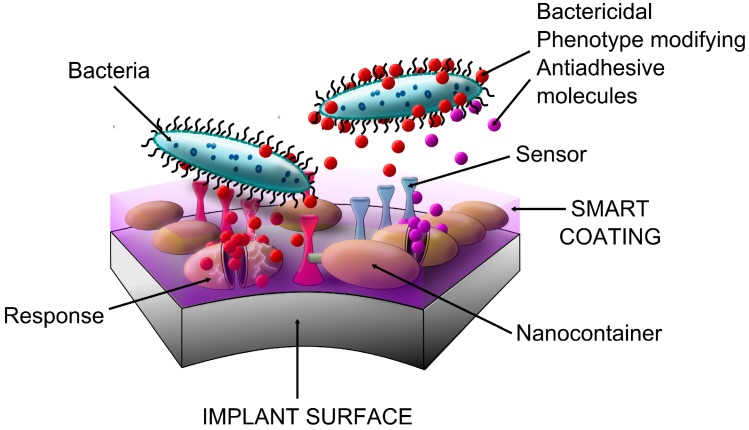
It is expected that the projected increased usage of implantable devices in medicine will result in a natural rise in the number of infections related to these cases. Some patients are unable to autonomously prevent formation of biofilm on implant surfaces. Suppression of the local peri-implant immune response is an important contributory factor. Substantial avascular scar tissue encountered during revision joint replacement surgery places these cases at an especially high risk of periprosthetic joint infection. A critical pathogenic event in the process of biofilm formation is bacterial adhesion. Prevention of biomaterial-associated infections should be concurrently focused on at least two targets: inhibition of biofilm formation and minimizing local immune response suppression. Current knowledge of antimicrobial surface treatments suitable for prevention of prosthetic joint infection is reviewed. Several surface treatment modalities have been proposed. Minimizing bacterial adhesion, biofilm formation inhibition, and bactericidal approaches are discussed. The ultimate anti-infective surface should be "smart" and responsive to even the lowest bacterial load. While research in this field is promising, there appears to be a great discrepancy between proposed and clinically implemented strategies, and there is urgent need for translational science focusing on this topic.
Figures
Similar articles
-
Antibacterial coating of implants in orthopaedics and trauma: a classification proposal in an evolving panorama.J Orthop Surg Res. 2015 Oct 1;10:157. doi: 10.1186/s13018-015-0294-5. J Orthop Surg Res. 2015. PMID: 26429342 Free PMC article. Review.
-
Zirconium Nitride Coating Reduced Staphylococcus epidermidis Biofilm Formation on Orthopaedic Implant Surfaces: An In Vitro Study.Clin Orthop Relat Res. 2019 Feb;477(2):461-466. doi: 10.1097/CORR.0000000000000568. Clin Orthop Relat Res. 2019. PMID: 30418277 Free PMC article.
-
Antibacterial coatings on titanium implants.J Biomed Mater Res B Appl Biomater. 2009 Oct;91(1):470-80. doi: 10.1002/jbm.b.31463. J Biomed Mater Res B Appl Biomater. 2009. PMID: 19637369 Review.
-
Emerging antibacterial biomaterial strategies for the prevention of peri-implant inflammatory diseases.Int J Oral Maxillofac Implants. 2011 May-Jun;26(3):553-60. Int J Oral Maxillofac Implants. 2011. PMID: 21691602 Review.
-
Antibacterial surfaces for biomedical devices.Expert Rev Med Devices. 2009 Sep;6(5):553-67. doi: 10.1586/erd.09.36. Expert Rev Med Devices. 2009. PMID: 19751126 Review.
Cited by
-
Understanding orthopedic infections through a different perspective: Microcalorimetry growth curves.Exp Ther Med. 2022 Apr;23(4):263. doi: 10.3892/etm.2022.11189. Epub 2022 Feb 4. Exp Ther Med. 2022. PMID: 35251329 Free PMC article.
-
Antibacterial coatings on orthopedic implants.Mater Today Bio. 2023 Feb 15;19:100586. doi: 10.1016/j.mtbio.2023.100586. eCollection 2023 Apr. Mater Today Bio. 2023. PMID: 36896412 Free PMC article. Review.
-
Can the Hydroxyapatite-Coated Skin-Penetrating Abutment for Bone Conduction Hearing Implants Integrate with the Surrounding Skin?Front Surg. 2015 Sep 14;2:45. doi: 10.3389/fsurg.2015.00045. eCollection 2015. Front Surg. 2015. PMID: 26442276 Free PMC article.
-
Pioneering nanomedicine in orthopedic treatment care: a review of current research and practices.Front Bioeng Biotechnol. 2024 May 27;12:1389071. doi: 10.3389/fbioe.2024.1389071. eCollection 2024. Front Bioeng Biotechnol. 2024. PMID: 38860139 Free PMC article. Review.
-
Modern Microbiological Methods to Detect Biofilm Formation in Orthopedy and Suggestions for Antibiotic Therapy, with Particular Emphasis on Prosthetic Joint Infection (PJI).Microorganisms. 2024 Jun 14;12(6):1198. doi: 10.3390/microorganisms12061198. Microorganisms. 2024. PMID: 38930580 Free PMC article. Review.
References
-
- Lentino J.R. Prosthetic joint infections: Bane of orthopedists, challenge for infectious disease specialists. Clin. Infect. Dis. 2003;36:1157–1161. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
