

Decreased occipital cortical glutamate levels in response to successful cognitive-behavioral therapy and pharmacotherapy for major depressive disorder
- PMID: 25116726
- PMCID: PMC4164203
- DOI: 10.1159/000361078
Decreased occipital cortical glutamate levels in response to successful cognitive-behavioral therapy and pharmacotherapy for major depressive disorder
Abstract
Background: Previous studies have demonstrated that antidepressant medication and electroconvulsive therapy increase occipital cortical γ-aminobutyric acid (GABA) in major depressive disorder (MDD), but a small pilot study failed to show a similar effect of cognitive-behavioral therapy (CBT) on occipital GABA. In light of these findings we sought to determine if baseline GABA levels predict treatment response and to broaden the analysis to other metabolites and neurotransmitters in this larger study.
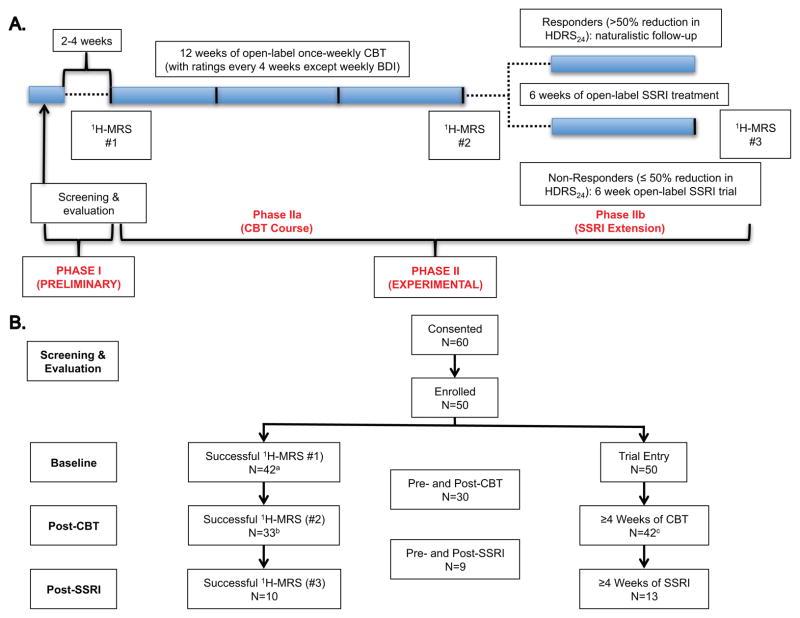
Methods: A total of 40 MDD outpatients received baseline proton magnetic resonance spectroscopy (1H-MRS), and 30 subjects completed both pre- and post-CBT 1H-MRS; 9 CBT nonresponders completed an open-label medication phase followed by an additional/3rd 1H-MRS. The magnitude of treatment response was correlated with occipital amino acid neurotransmitter levels.
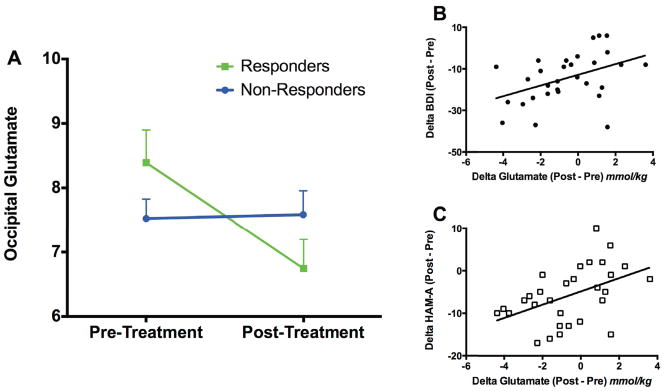
Results: Baseline GABA did not predict treatment outcome. Furthermore, there was no significant effect of CBT on GABA levels. However, we found a significant group × time interaction (F1, 28 = 6.30, p = 0.02), demonstrating reduced glutamate in CBT responders, with no significant glutamate change in CBT nonresponders.
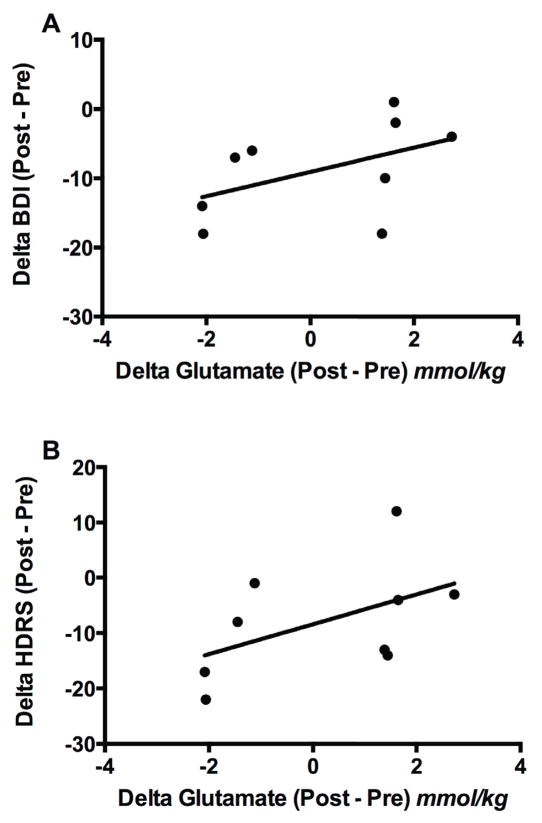
Conclusions: These findings corroborate the lack of effect of successful CBT on occipital cortical GABA levels in a larger sample. A reduction in glutamate levels following treatment, on the other hand, correlated with successful CBT and antidepressant medication response. Based on this finding and other reports, decreased occipital glutamate may be an antidepressant response biomarker. Healthy control comparator and nonintervention groups may shed light on the sensitivity and specificity of these results.
Conflict of interest statement
Conflict of interest statement: Dr. Sanacora has received consulting fees from AstraZeneca, Avanier Pharmaceuticals, Bristol-Myers Squibb, Eli Lilly & Co., Hoffman La-Roche, Naurex and Noven Pharmaceuticals over the last 36 months. He has also received additional grant support from AstraZeneca, Bristol-Myers Squibb, Hoffman La-Roche, Eli Lilly & Co., Janssen, Merck & Co. and Naurex over the last 36 months. In addition he is a co-inventor on filed patent application by Yale University (PCTWO06108055A1) and holds shares in BioHaven Pharmaceuticals Holding Company. Dr. Abdallah has received consulting fees from Genentech. None of the other authors report any potential conflict of interests.
Figures
References
-
- Kessler RC, Berglund P, Demler O, Jin R, Koretz D, Merikangas KR, Rush AJ, Walters EE, Wang PS. The epidemiology of major depressive disorder: Results from the National Comorbidity Survey Replication (NCS-R) JAMA. 2003;289:3095–3105. - PubMed
-
- Ustun TB, Ayuso-Mateos JL, Chatterji S, Mathers C, Murray CJ. Global burden of depressive disorders in the year 2000. Br J Psychiatry. 2004;184:386–392. - PubMed
-
- Ormel J, Petukhova M, Chatterji S, Aguilar-Gaxiola S, Alonso J, Angermeyer MC, Bromet EJ, Burger H, Demyttenaere K, de Girolamo G, Haro JM, Hwang I, Karam E, Kawakami N, Lepine JP, Medina-Mora ME, Posada-Villa J, Sampson N, Scott K, Ustun TB, Von Korff M, Williams DR, Zhang M, Kessler RC. Disability and treatment of specific mental and physical disorders across the world. Br J Psychiatry. 2008;192:368–375. - PMC - PubMed
-
- American Psychiatric Association. Practice Guideline for the Treatment of Patients with Major Depressive Disorder. 2. Washington, D.C: American Psychiatric Association; 2000.
-
- Simons AD, Murphy GE, Levine JL, Wetzel RD. Cognitive therapy and pharmacotherapy for depression. Sustained improvement over one year. Arch Gen Psychiatry. 1986;43:43–48. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- T32-DA022975/DA/NIDA NIH HHS/United States
- R01 DA021785/DA/NIDA NIH HHS/United States
- T32 MH19961/MH/NIMH NIH HHS/United States
- UL1 TR000142/TR/NCATS NIH HHS/United States
- K23 MH101498/MH/NIMH NIH HHS/United States
- R01 MH071676-05/MH/NIMH NIH HHS/United States
- T32 DA022975/DA/NIDA NIH HHS/United States
- R21 AA018210/AA/NIAAA NIH HHS/United States
- K02 MH076222/MH/NIMH NIH HHS/United States
- T32 MH019961/MH/NIMH NIH HHS/United States
- R01 MH071676/MH/NIMH NIH HHS/United States
- K02 MH076222-04/MH/NIMH NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
