

Effect of flexible sigmoidoscopy screening on colorectal cancer incidence and mortality: a randomized clinical trial
- PMID: 25117129
- PMCID: PMC4495882
- DOI: 10.1001/jama.2014.8266
Effect of flexible sigmoidoscopy screening on colorectal cancer incidence and mortality: a randomized clinical trial
Erratum in
- JAMA. 2014 Sep 3;312(9):964
Abstract
Importance: Colorectal cancer is a major health burden. Screening is recommended in many countries.
Objective: To estimate the effectiveness of flexible sigmoidoscopy screening on colorectal cancer incidence and mortality in a population-based trial.
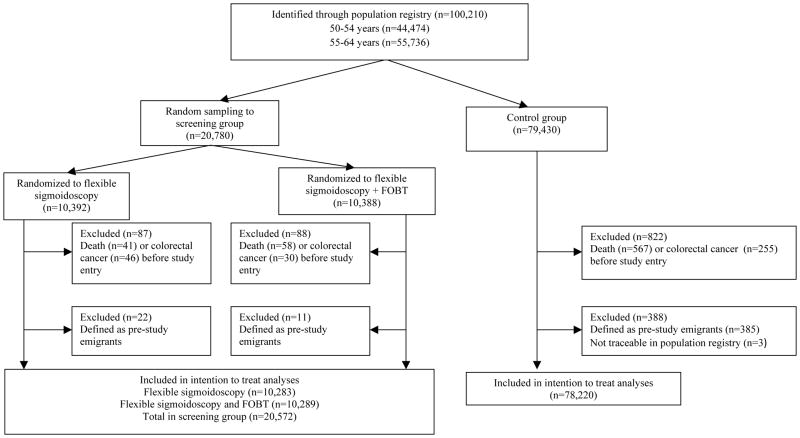
Design, setting, and participants: Randomized clinical trial of 100,210 individuals aged 50 to 64 years, identified from the population of Oslo city and Telemark County, Norway. Screening was performed in 1999-2000 (55-64-year age group) and in 2001 (50-54-year age group), with follow-up ending December 31, 2011. Of those selected, 1415 were excluded due to prior colorectal cancer, emigration, or death, and 3 could not be traced in the population registry.
Interventions: Participants randomized to the screening group were invited to undergo screening. Within the screening group, participants were randomized 1:1 to receive once-only flexible sigmoidoscopy or combination of once-only flexible sigmoidoscopy and fecal occult blood testing (FOBT). Participants with positive screening test results (cancer, adenoma, polyp ≥10 mm, or positive FOBT) were offered colonoscopy. The control group received no intervention.
Main outcomes and measures: Colorectal cancer incidence and mortality.
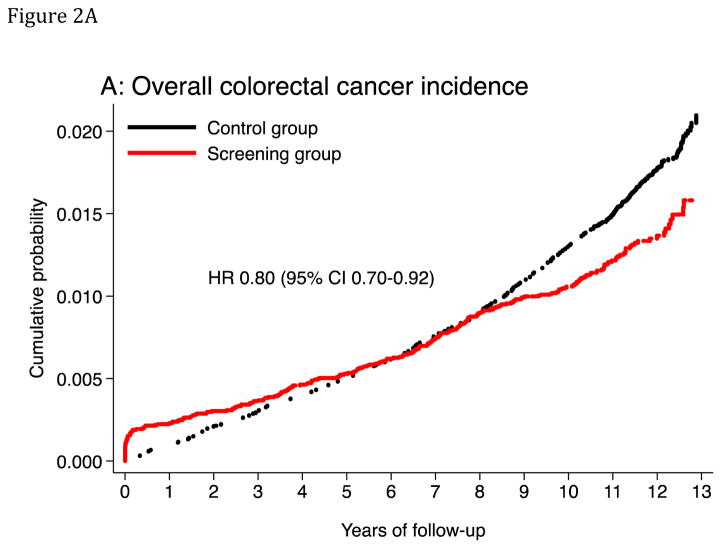
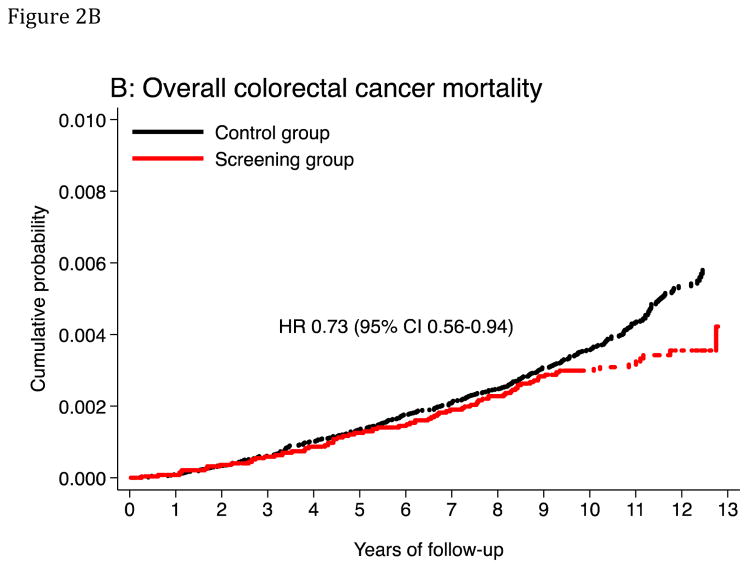
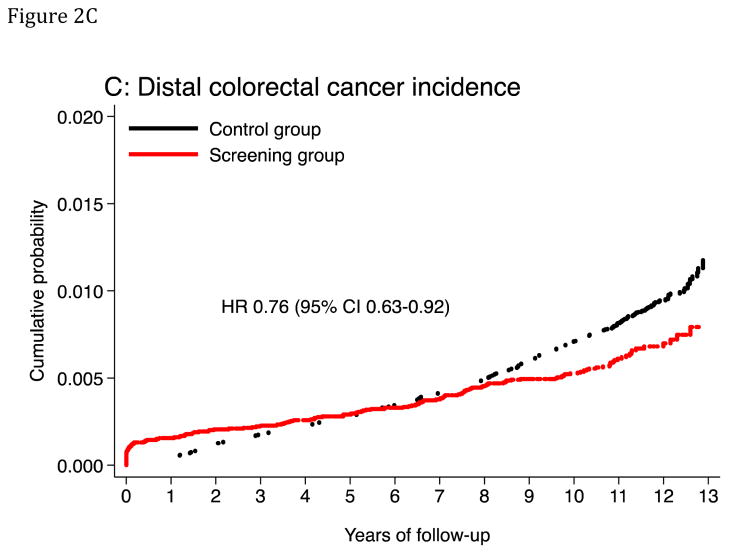
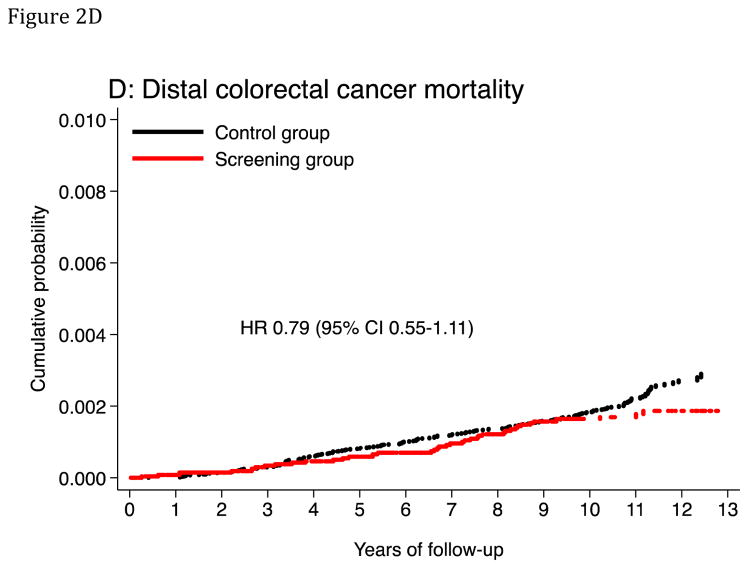
Results: A total of 98,792 participants were included in the intention-to-screen analyses, of whom 78,220 comprised the control group and 20,572 comprised the screening group (10,283 randomized to receive a flexible sigmoidoscopy and 10,289 to receive flexible sigmoidoscopy and FOBT). Adherence with screening was 63%. After a median of 10.9 years, 71 participants died of colorectal cancer in the screening group vs 330 in the control group (31.4 vs 43.1 deaths per 100,000 person-years; absolute rate difference, 11.7 [95% CI, 3.0-20.4]; hazard ratio [HR], 0.73 [95% CI, 0.56-0.94]). Colorectal cancer was diagnosed in 253 participants in the screening group vs 1086 in the control group (112.6 vs 141.0 cases per 100,000 person-years; absolute rate difference, 28.4 [95% CI, 12.1-44.7]; HR, 0.80 [95% CI, 0.70-0.92]). Colorectal cancer incidence was reduced in both the 50- to 54-year age group (HR, 0.68; 95% CI, 0.49-0.94) and the 55- to 64-year age group (HR, 0.83; 95% CI, 0.71-0.96). There was no difference between the flexible sigmoidoscopy only vs the flexible sigmoidoscopy and FOBT screening groups.
Conclusions and relevance: In Norway, once-only flexible sigmoidoscopy screening or flexible sigmoidoscopy and FOBT reduced colorectal cancer incidence and mortality on a population level compared with no screening. Screening was effective both in the 50- to 54-year and the 55- to 64-year age groups.
Trial registration: clinicaltrials.gov Identifier: NCT00119912.
Conflict of interest statement
Conflict of interest disclosure: Michael Bretthauer is member of the European scientific advisory board of Exact Sciences and has received equipment for testing in scientific studies from Olympus, Fujinon, Falk Phgroup and CCS Healthcare. Holme, Løberg, Skovlund, Schneede, Aas, Hoff, Eide, Tveit, Kalager, Hernán report no conflicts of interest.
Figures
Comment in
-
Flexible sigmoidoscopy for colorectal cancer screening: more evidence, persistent ironies.JAMA. 2014 Aug 13;312(6):601-2. doi: 10.1001/jama.2014.8613. JAMA. 2014. PMID: 25117127 No abstract available.
-
Colorectal cancer and the effect of flexible sigmoidoscopy screening.JAMA. 2014 Dec 10;312(22):2411. doi: 10.1001/jama.2014.14692. JAMA. 2014. PMID: 25490337 No abstract available.
-
Colorectal cancer and the effect of flexible sigmoidoscopy screening--reply.JAMA. 2014 Dec 10;312(22):2411-2. doi: 10.1001/jama.2014.14695. JAMA. 2014. PMID: 25490338 No abstract available.
-
Invitation for flexible sigmoidoscopy screening reduced colorectal cancer and colorectal cancer mortality.Ann Intern Med. 2014 Dec 16;161(12):JC2. doi: 10.7326/0003-4819-161-12-201412160-02002. Ann Intern Med. 2014. PMID: 25506874 No abstract available.
-
Response to Cox letter.N Z Med J. 2016 Dec 2;129(1446):116-118. N Z Med J. 2016. PMID: 27906930 No abstract available.
References
-
- Ferlay J, Soerjomataram I, Ervik M, et al. GLOBOCAN 2012 v1.0, Cancer Incidence and Mortality Worldwide: IARC CancerBase No. 11 [Internet] Lyon, France: International Agency for Research on Cancer; 2013. [Accessed March 11th 2014]. http://globocan.iarc.fr/Pages/online.aspx.
-
- Muto T, Bussey HJ, Morson BC. The evolution of cancer of the colon and rectum. Cancer. 1975;36(6):2251–2270. - PubMed
-
- Levin B, Lieberman DA, McFarland B, et al. Screening and surveillance for the early detection of colorectal cancer and adenomatous polyps, 2008: a joint guideline from the American Cancer Society, the US Multi-Society Task Force on Colorectal Cancer, and the American College of Radiology. Gastroenterology. 2008;134(5):1570–1595. - PubMed
-
- West NJ, Boustiere C, Fischbach W, et al. Colorectal cancer screening in Europe: differences in approach; similar barriers to overcome. Int J Colorectal Dis. 2009;24(7):731–740. - PubMed
-
- Atkin WS, Edwards R, Kralj-Hans I, et al. Once-only flexible sigmoidoscopy screening in prevention of colorectal cancer: a multicentre randomised controlled trial. Lancet. 2010;375(9726):1624–1633. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
