

Hand sanitiser provision for reducing illness absences in primary school children: a cluster randomised trial
- PMID: 25117155
- PMCID: PMC4130492
- DOI: 10.1371/journal.pmed.1001700
Hand sanitiser provision for reducing illness absences in primary school children: a cluster randomised trial
Abstract
Background: The potential for transmission of infectious diseases offered by the school environment are likely to be an important contributor to the rates of infectious disease experienced by children. This study aimed to test whether the addition of hand sanitiser in primary school classrooms compared with usual hand hygiene would reduce illness absences in primary school children in New Zealand.
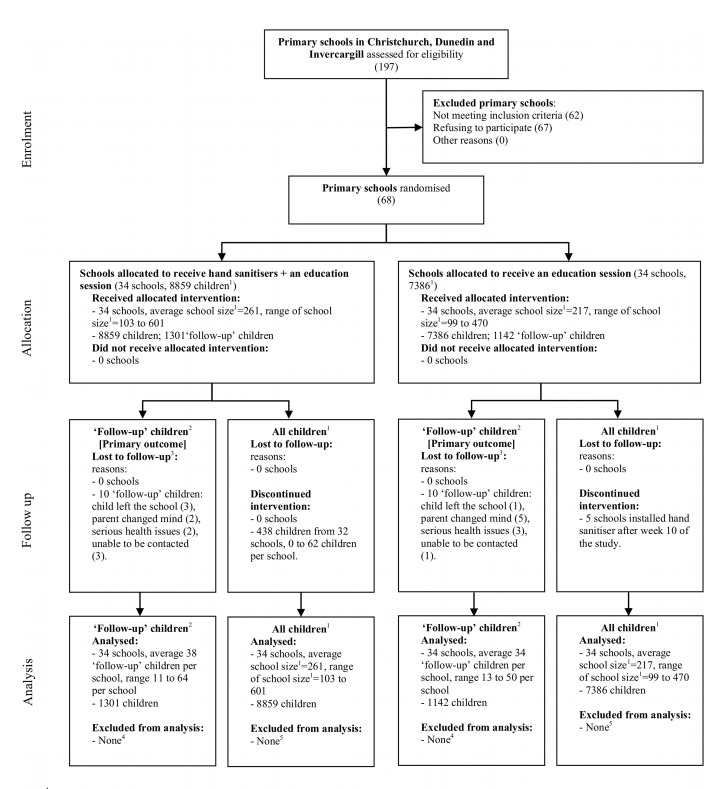
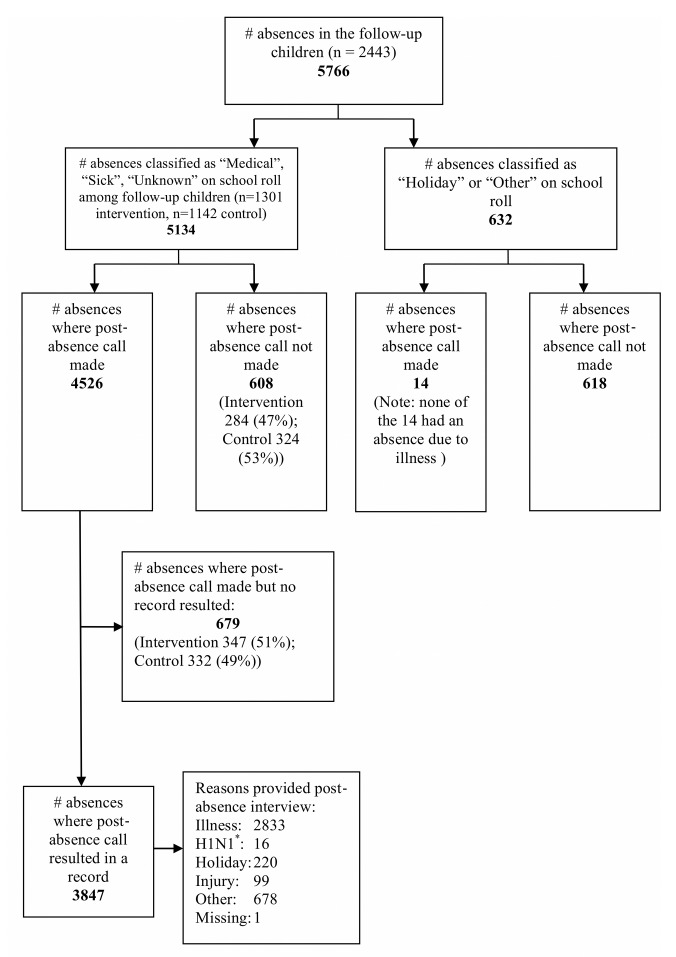
Methods and findings: This parallel-group cluster randomised trial took place in 68 primary schools, where schools were allocated using restricted randomisation (1:1 ratio) to the intervention or control group. All children (aged 5 to 11 y) in attendance at participating schools received an in-class hand hygiene education session. Schools in the intervention group were provided with alcohol-based hand sanitiser dispensers in classrooms for the winter school terms (27 April to 25 September 2009). Control schools received only the hand hygiene education session. The primary outcome was the number of absence episodes due to any illness among 2,443 follow-up children whose caregivers were telephoned after each absence from school. Secondary outcomes measured among follow-up children were the number of absence episodes due to specific illness (respiratory or gastrointestinal), length of illness and illness absence episodes, and number of episodes where at least one other member of the household became ill subsequently (child or adult). We also examined whether provision of sanitiser was associated with experience of a skin reaction. The number of absences for any reason and the length of the absence episode were measured in all primary school children enrolled at the schools. Children, school administrative staff, and the school liaison research assistants were not blind to group allocation. Outcome assessors of follow-up children were blind to group allocation. Of the 1,301 and 1,142 follow-up children in the hand sanitiser and control groups, respectively, the rate of absence episodes due to illness per 100 child-days was similar (1.21 and 1.16, respectively, incidence rate ratio 1.06, 95% CI 0.94 to 1.18). The provision of an alcohol-based hand sanitiser dispenser in classrooms was not effective in reducing rates of absence episodes due to respiratory or gastrointestinal illness, the length of illness or illness absence episodes, or the rate of subsequent infection for other members of the household in these children. The percentage of children experiencing a skin reaction was similar (10.4% hand sanitiser versus 10.3% control, risk ratio 1.01, 95% CI 0.78 to 1.30). The rate or length of absence episodes for any reason measured for all children also did not differ between groups. Limitations of the study include that the study was conducted during an influenza pandemic, with associated public health messaging about hand hygiene, which may have increased hand hygiene among all children and thereby reduced any additional effectiveness of sanitiser provision. We did not quite achieve the planned sample size of 1,350 follow-up children per group, although we still obtained precise estimates of the intervention effects. Also, it is possible that follow-up children were healthier than non-participating eligible children, with therefore less to gain from improved hand hygiene. However, lack of effectiveness of hand sanitiser provision on the rate of absences among all children suggests that this may not be the explanation.
Conclusions: The provision of hand sanitiser in addition to usual hand hygiene in primary schools in New Zealand did not prevent disease of severity sufficient to cause school absence.
Trial registration: Australian New Zealand Clinical Trials Registry ACTRN12609000478213. Please see later in the article for the Editors' Summary.
Conflict of interest statement
The authors have declared that no competing interests exist. All authors affirm that they are not involved in any other trials on the same or a related intervention.
Figures
References
-
- Murray CJ, Vos T, Lozano R, Naghavi M, Flaxman AD, et al. (2012) Disability-adjusted life years (DALYs) for 291 diseases and injuries in 21 regions, 1990–2010: a systematic analysis for the Global Burden of Disease Study 2010. Lancet 380: 2197–2223. - PubMed
-
- Baker MG, Barnard LT, Kvalsvig A, Verrall A, Zhang J, et al. (2012) Increasing incidence of serious infectious diseases and inequalities in New Zealand: a national epidemiological study. Lancet 379: 1112–1119. - PubMed
-
- Neuzil KM, Hohlbein C, Zhu Y (2002) Illness among schoolchildren during influenza season: effect on school absenteeism, parental absenteeism from work, and secondary illness in families. Arch Pediatr Adolesc Med 156: 986–991. - PubMed
-
- Pittet D (2005) Clean care is safer care: the first global challenge of the WHO World Alliance for Patient Safety. Infect Control Hosp Epidemiol 26: 891–894. - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
