

Risk of Lower Extremity Injury in a Military Cadet Population After a Supervised Injury-Prevention Program
- PMID: 25117875
- PMCID: PMC5224732
- DOI: 10.4085/1062-6050-49.5.22
Risk of Lower Extremity Injury in a Military Cadet Population After a Supervised Injury-Prevention Program
Abstract
Context: Specific movement patterns have been identified as possible risk factors for noncontact lower extremity injuries. The Dynamic Integrated Movement Enhancement (DIME) was developed to modify these movement patterns to decrease injury risk.
Objective: To determine if the DIME is effective for preventing lower extremity injuries in US Military Academy (USMA) cadets.
Design: Cluster-randomized controlled trial.
Setting: Cadet Basic Training at USMA.
Patients or other participants: Participants were 1313 cadets (1070 men, 243 women).
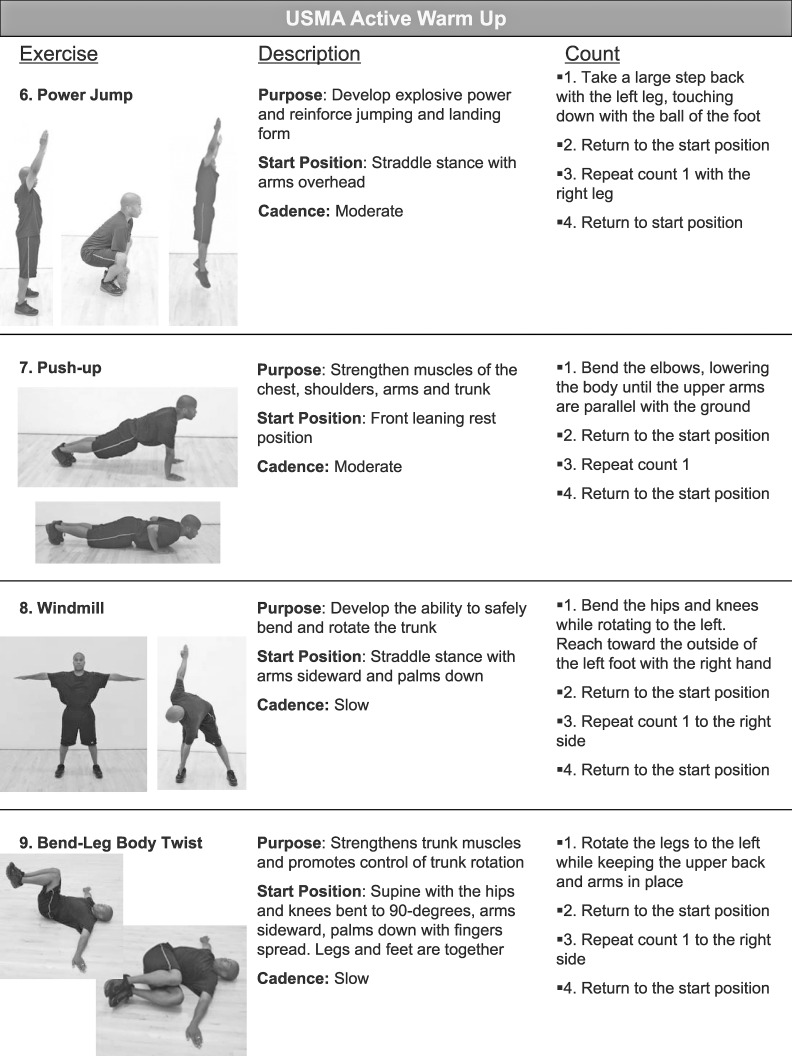
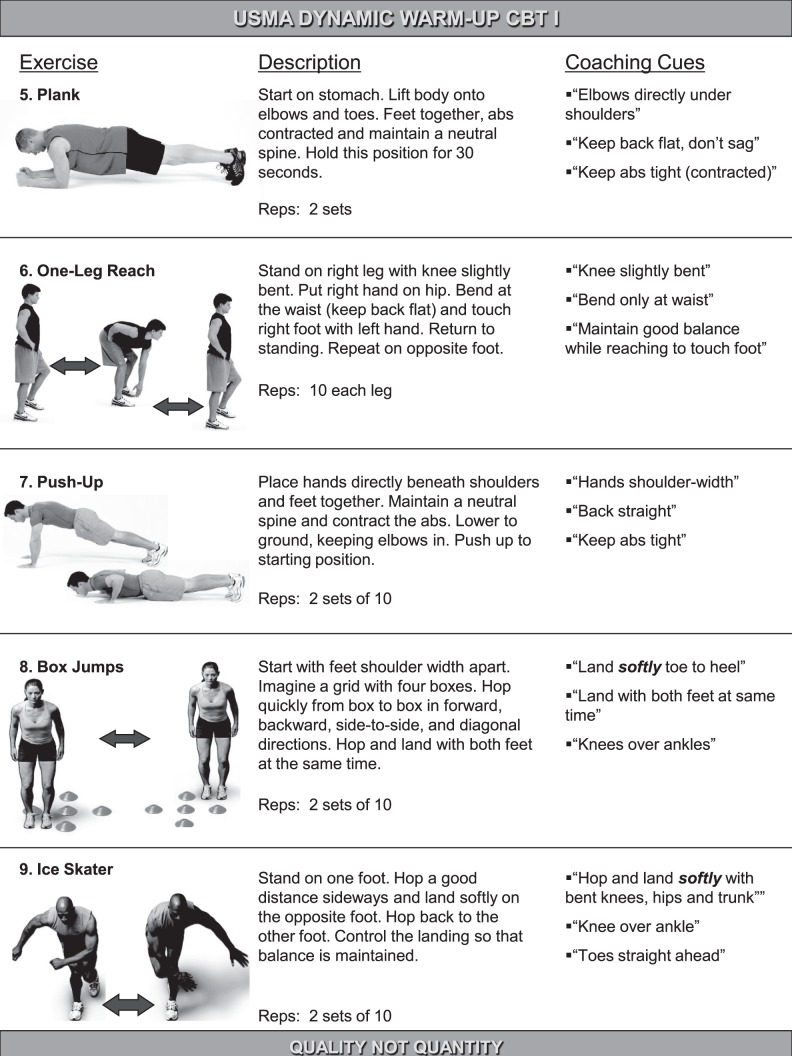
Intervention(s): Participants were cluster randomized to 3 groups. The active warm-up (AWU) group performed standard Army warm-up exercises. The DIME groups were assigned to a DIME cadre-supervised (DCS) group or a DIME expert-supervised (DES) group; the former consisted of cadet supervision and the latter combined cadet and health professional supervision. Groups performed exercises 3 times weekly for 6 weeks.
Main outcome measure(s): Cumulative risk of lower extremity injury was the primary outcome. We gathered data during Cadet Basic Training and for 9 months during the subsequent academic year. Risk ratios and 95% confidence intervals (CIs) were calculated to compare groups.
Results: No differences were seen between the AWU and the combined DIME (DCS and DES) groups during Cadet Basic Training or the academic year. During the academic year, lower extremity injury risk in the DES group decreased 41% (relative risk [RR] = 0.59; 95% CI = 0.38, 0.93; P = .02) compared with the DCS group; a nonsignificant 25% (RR = 0.75; 95% CI = 0.49, 1.14; P = .18) decrease occurred in the DES group compared with the AWU group. Finally, there was a nonsignificant 27% (RR = 1.27; 95% CI = 0.90, 1.78; P = .17) increase in injury risk during the academic year in the DCS group compared with the AWU group.
Conclusions: We observed no differences in lower extremity injury risk between the AWU and combined DIME groups. However, the magnitude and direction of the risk ratios in the DES group compared with the AWU group, although not statistically significant, indicate that professional supervision may be a factor in the success of injury-prevention programs.
Keywords: Dynamic Integrated Movement Enhancement; exercises; warm-ups.
Figures



Similar articles
-
The Effects of an Injury Prevention Program on Landing Biomechanics Over Time.Am J Sports Med. 2016 Mar;44(3):767-76. doi: 10.1177/0363546515621270. Epub 2016 Jan 20. Am J Sports Med. 2016. PMID: 26792707 Clinical Trial.
-
Effect of a Lower Extremity Preventive Training Program on Physical Performance Scores in Military Recruits.J Strength Cond Res. 2017 Nov;31(11):3146-3157. doi: 10.1519/JSC.0000000000001792. J Strength Cond Res. 2017. PMID: 29068865 Clinical Trial.
-
Soccer-specific warm-up and lower extremity injury rates in collegiate male soccer players.J Athl Train. 2013 Nov-Dec;48(6):782-9. doi: 10.4085/1062-6050-48.4.08. Epub 2013 Jul 12. J Athl Train. 2013. PMID: 23848519 Free PMC article.
-
Rationale and implementation of anterior cruciate ligament injury prevention warm-up programs in female athletes.J Strength Cond Res. 2011 Jan;25(1):271-85. doi: 10.1519/JSC.0b013e3181fb4a5a. J Strength Cond Res. 2011. PMID: 21116195 Review.
-
Physical training in boots and running shoes: a historical comparison of injury incidence in basic combat training.Mil Med. 2015 Mar;180(3):321-8. doi: 10.7205/MILMED-D-14-00337. Mil Med. 2015. PMID: 25735024 Review.
Cited by
-
Toward more reliable stability measurements in stance: recommendations for number of measurements, foot position and feedback -- a cross-sectional study among servicemen.Mil Med Res. 2019 Jul 12;6(1):21. doi: 10.1186/s40779-019-0212-y. Mil Med Res. 2019. PMID: 31296263 Free PMC article.
-
Barriers and facilitators to implementation of musculoskeletal injury mitigation programmes for military service members around the world: a scoping review.Inj Prev. 2023 Nov 27;29(6):461-473. doi: 10.1136/ip-2023-044905. Inj Prev. 2023. PMID: 37620010 Free PMC article.
-
Pre-academy knee pain as a predictor of overuse knee injuries in first-year military cadets.BMJ Mil Health. 2025 Aug 11:military-2025-003033. doi: 10.1136/military-2025-003033. Online ahead of print. BMJ Mil Health. 2025. PMID: 40789695 Free PMC article.
-
Do Exercise-Based Prevention Programs Reduce Injury in Endurance Runners? A Systematic Review and Meta-Analysis.Sports Med. 2024 May;54(5):1249-1267. doi: 10.1007/s40279-024-01993-7. Epub 2024 Jan 23. Sports Med. 2024. PMID: 38261240 Free PMC article.
-
The mechanism and cause of anterior cruciate ligament tear in the Korean military environment.Knee Surg Relat Res. 2019 Nov 28;31(1):13. doi: 10.1186/s43019-019-0015-1. Knee Surg Relat Res. 2019. PMID: 32660592 Free PMC article.
References
-
- Jones BH, Canham-Chervak M, Sleet DA. . An evidence-based public health approach to injury priorities and prevention. Am J Prev Med. 2010; 38 1 suppl: S1– S10. - PubMed
-
- Veigel JD, Pleacher MD. . Injury prevention in youth sports. Curr Sports Med Rep. 2008; 7 6: 348– 352. - PubMed
-
- Finch CF, Ullah S, McIntosh AS. . Combining epidemiology and biomechanics in sports injury prevention research: a new approach for selecting suitable controls. Sports Med. 2011; 41 1: 59– 72. - PubMed
-
- Bullock SH, Jones BH, Gilchrist J, Marshall SW. . Prevention of physical training-related injuries: recommendations for the military and other active populations based on expedited systematic reviews. Am J Prev Med. 2010; 38 suppl 1: S156– S181. - PubMed
-
- Hewett TE, Johnson DL. . ACL prevention programs: fact or fiction? Orthopedics. 2010; 33 1: 36– 39. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
