

Mechanisms of disseminated cancer cell dormancy: an awakening field
- PMID: 25118602
- PMCID: PMC4230700
- DOI: 10.1038/nrc3793
Mechanisms of disseminated cancer cell dormancy: an awakening field
Abstract
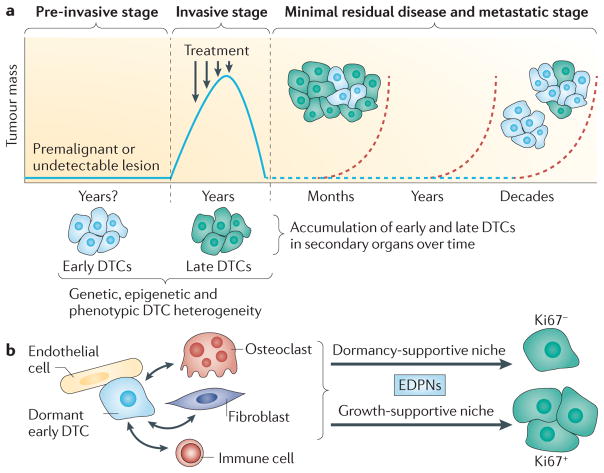
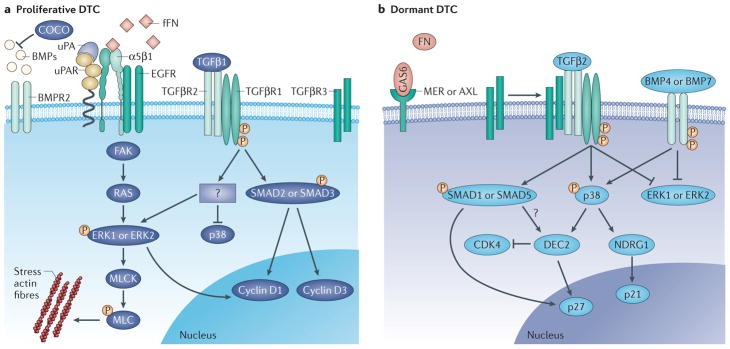
Metastases arise from residual disseminated tumour cells (DTCs). This can happen years after primary tumour treatment because residual tumour cells can enter dormancy and evade therapies. As the biology of minimal residual disease seems to diverge from that of proliferative lesions, understanding the underpinnings of this new cancer biology is key to prevent metastasis. Analysis of approximately 7 years of literature reveals a growing focus on tumour and normal stem cell quiescence, extracellular and stromal microenvironments, autophagy and epigenetics as mechanisms that dictate tumour cell dormancy. In this Review, we attempt to integrate this information and highlight both the weaknesses and the strengths in the field to provide a framework to understand and target this crucial step in cancer progression.
Conflict of interest statement
The authors declare
Figures

References
-
- Klein CA. Framework models of tumor dormancy from patient-derived observations. Curr Opin Genet Dev. 2010;21:42–49. - PubMed
-
- Goss PE, Chambers AF. Does tumour dormancy offer a therapeutic target? Nature Rev Cancer. 2010;10:871–877. - PubMed
-
- Klein CA. Selection and adaptation during metastatic cancer progression. Nature. 2013;501:365–372. - PubMed
-
- Demicheli R, et al. Breast cancer recurrence dynamics following adjuvant CMF is consistent with tumor dormancy and mastectomy-driven acceleration of the metastatic process. Ann Oncol. 2005;16:1449–1457. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
