

Use of oversized injectable valves in growing children for total repair of right ventricular outflow tract anomalies (preliminary results)
- PMID: 25120389
- PMCID: PMC4120499
- DOI: 10.14503/THIJ-13-3359
Use of oversized injectable valves in growing children for total repair of right ventricular outflow tract anomalies (preliminary results)
Abstract
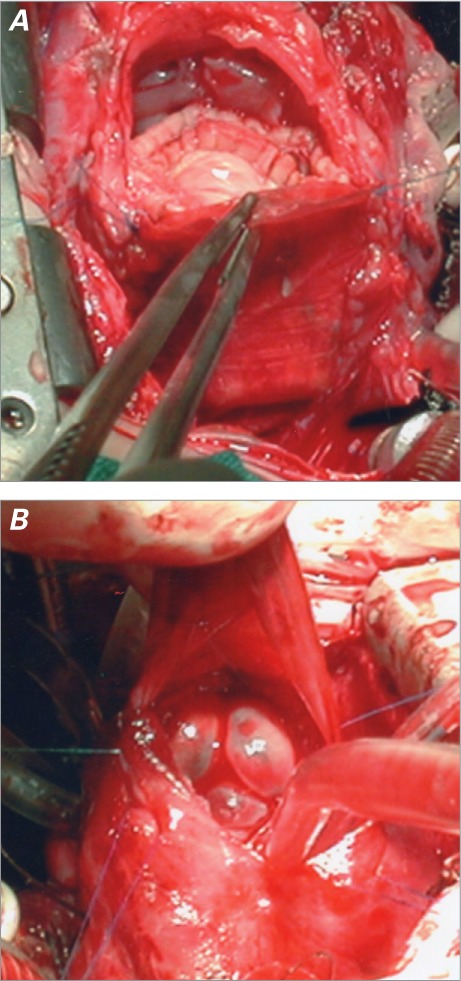
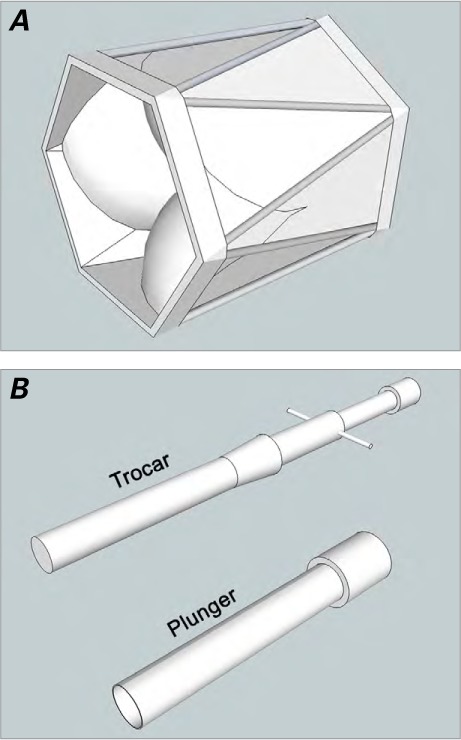
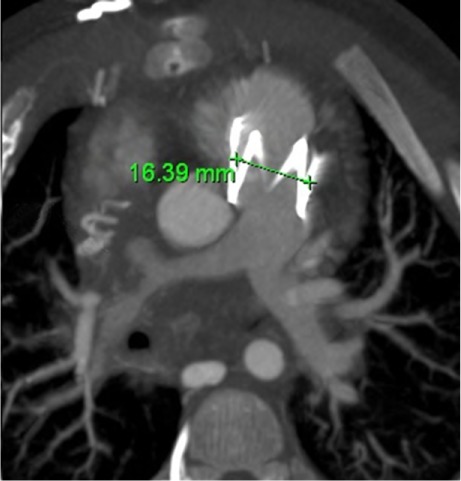
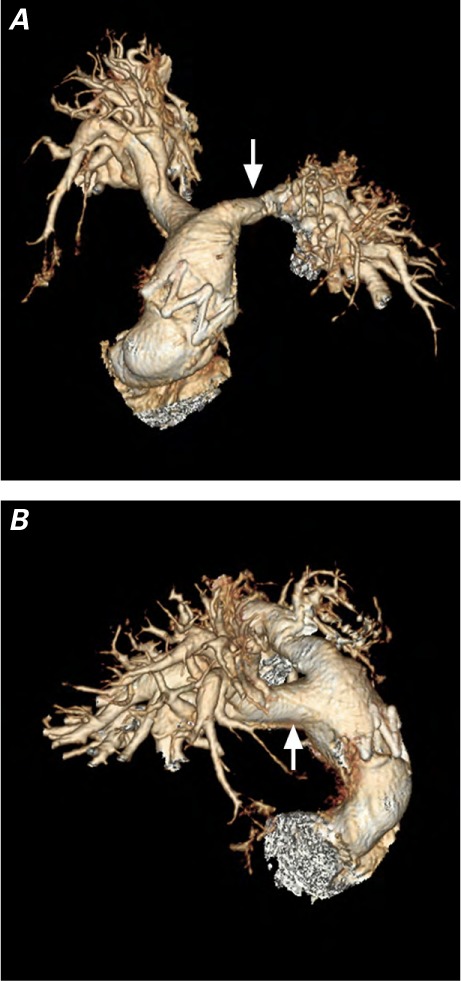
Right ventricular outflow tract surgery was originally confined to transannular patching, in the belief that pulmonary regurgitation was well tolerated. Because follow-up evaluations revealed the deleterious effects of pulmonary regurgitation, surgery today aims to spare or replace the valve. Available replacement devices have short lifetimes, considering growth mismatch in children. We hypothesize that oversizing the right infundibulum anticipates growth and that a squeezed prosthesis can complete the expansion process. The No-React® Injectable BioPulmonic Valve is designed for right infundibular surgery in adults, and hundreds of implants have shown promising results. We used this device for surgery in babies, with the addition of an innovative oversizing technique. This study evaluates our preliminary results and investigates whether such a technique might reduce growth mismatch. From September 2010 through July 2012, we implanted 11 injectable pulmonic valves. The median age of our patients was 23 months. After opening the right infundibulum, we enlarged it as much as possible with a wide patch. Before completing the patch suture, we injected an oversized valve. No problems occurred during surgery. No major insufficiency or leak was observed. We conclude that prostheses can be quite oversized and perform well even when not completely expanded. Oversized injectable pulmonic valves, shrunken to a smaller diameter, enabled the implantation of a device wider than otherwise possible, without affecting performance. Moreover, the prosthesis tended to return to its original size following growth, thereby reducing growth mismatch. Longer follow-up and larger numbers of patients are needed for verification.
Keywords: Bioprosthesis; cardiac surgical procedures/methods/pediatric; child; constriction, pathologic; heart defects, congenital; heart valve prosthesis implantation; infant; prostheses and implants; pulmonary regurgitation; pulmonary valve insufficiency; pulmonary valve/abnormalities/surgery; right ventricular outflow tract; time factors; treatment outcome; ventricular outflow obstructions.
Figures
References
-
- Katz NM, Blackstone EH, Kirklin JW, Pacifico AD, Bargeron LM., Jr. Late survival and symptoms after repair of tetralogy of Fallot. Circulation. 1982;65(2):403–10. - PubMed
-
- Bacha EA, Scheule AM, Zurakowski D, Erickson LC, Hung J, Lang P et al. Long-term results after early primary repair of tetralogy of Fallot. J Thorac Cardiovasc Surg. 2001;122(1):154–61. - PubMed
-
- Bacha E. Valve-sparing options in tetralogy of Fallot surgery. Semin Thorac Cardiovasc Surg Pediatr Card Surg Annu. 2012;15(1):24–6. - PubMed
-
- Bouzas B, Kilner PJ, Gatzoulis MA. Pulmonary regurgitation: not a benign lesion. Eur Heart J. 2005;26(5):433–9. - PubMed
-
- Frigiola A, Tsang V, Nordmeyer J, Lurz P, van Doorn C, Taylor AM et al. Current approaches to pulmonary regurgitation. Eur J Cardiothorac Surg. 2008;34(3):576–82. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
