

Quantitative phenotyping of bone fracture repair: a review
- PMID: 25120907
- PMCID: PMC4119206
- DOI: 10.1038/bonekey.2014.45
Quantitative phenotyping of bone fracture repair: a review
Abstract
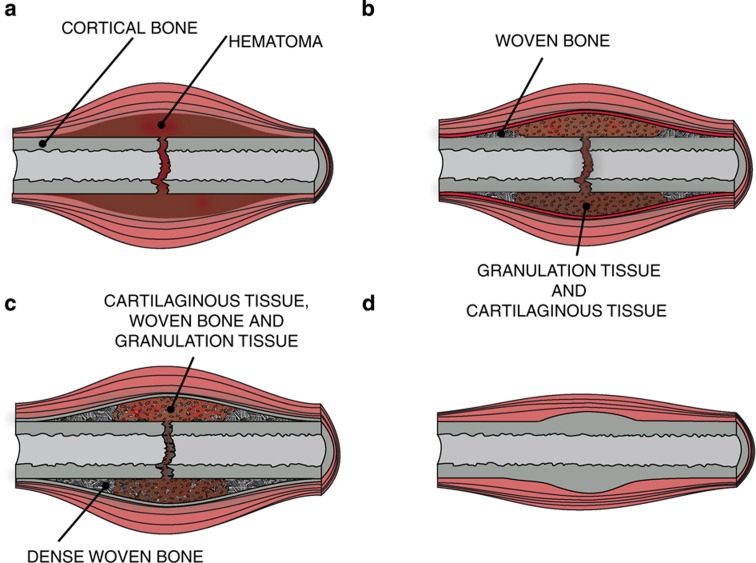
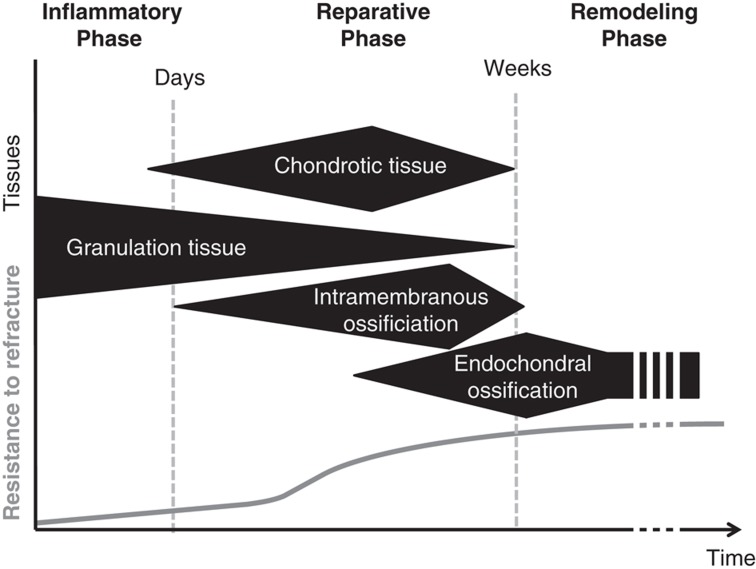
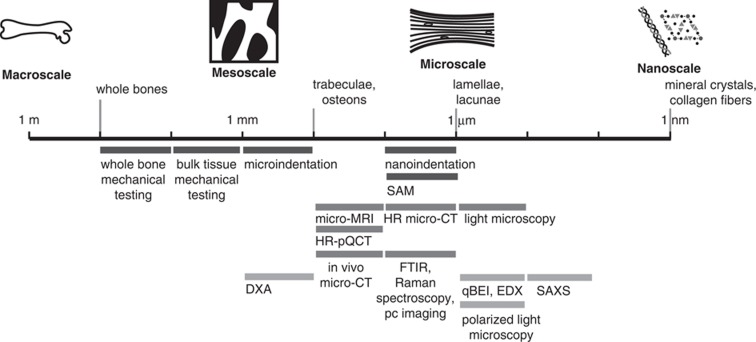
Fracture repair is a complex process that involves the interaction of numerous molecular factors, cell lineages and tissue types. These biological processes allow for an impressive feat of engineering: an elastic soft callus is progressively replaced by a more rigid and mineralized callus. During this reparative phase, the healing bone is exposed to a risk of re-fracture. Bone volume and bone quality are the two major factors determining the strength of the callus. Although both factors are important, often only bone volume is analyzed and reported in preclinical studies. Recent developments in techniques for examining bone quality in the callus will enable the rapid and detailed analysis of its material properties and its microstructure. This review aims to give an overview of the methods available for quantitatively phenotyping the bone callus in preclinical studies such as Raman spectroscopy, nanoindentation, scanning acoustic microscopy, in vivo micro-computed tomography (micro-CT) and high-resolution micro-CT. Consolidated and emerging experimental methods are described with a focus on their applicability, and with examples of their utilization.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- Sfeir C, Ho L, Doll BA, Azari K, Hollinger JO. Fracture repair. In: Lieberman JR, Friedlaender GE (eds) Bone Regeneration and Repair: Biology and Clinical Applications Humana Press: Totowa, NJ, USA, 2005;21–44.
-
- Aaron RK, Ciombor DM, Wang S, Simon B. Clinical biophysics: the promotion of skeletal repair by physical forces. Ann N Y Acad Sci 2006; 1068:513–531. - PubMed
-
- Little DG, Ramachandran M, Schindeler A. The anabolic and catabolic responses in bone repair. J Bone Joint Surg Br 2007; 89:425–433. - PubMed
-
- Liu Y, Manjubala I, Schell H, Epari DR, Roschger P, Duda GN et al. Size and habit of mineral particles in bone and mineralized callus during bone healing in sheep. J Bone Miner Res 2010; 25:2029–2038. - PubMed
-
- Galvis L, Mehta M, Masic A, Dunlop JWC, Duda G, Fratzl P. Collagen orientation during early stages of bone fracture healing investigated by polarized raman imaging. In: Champion PM, Ziegler LD (eds) XXII International Conference on Raman Spectroscopy Amer Inst Physics: Boston, MA, USA, 2010;406–407.
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources