

Awakening and withdrawal of life-sustaining treatment in cardiac arrest survivors treated with therapeutic hypothermia*
- PMID: 25121961
- PMCID: PMC4428607
- DOI: 10.1097/CCM.0000000000000540
Awakening and withdrawal of life-sustaining treatment in cardiac arrest survivors treated with therapeutic hypothermia*
Abstract
Objectives: To characterize the prevalence of withdrawal of life-sustaining treatment, as well as the time to awakening, short-term neurologic outcomes, and cause of death in comatose survivors of out-of-hospital resuscitated cardiopulmonary arrests treated with therapeutic hypothermia.
Design: Single center, prospective observational cohort study of consecutive patients with out-of-hospital cardiopulmonary arrests.
Setting: Academic tertiary care hospital and level one trauma center in Minneapolis, MN.
Patients: Adults with witnessed, nontraumatic, out-of-hospital cardiopulmonary arrests regardless of initial electrocardiographic rhythm with return of spontaneous circulation who were admitted to an ICU.
Interventions: None.
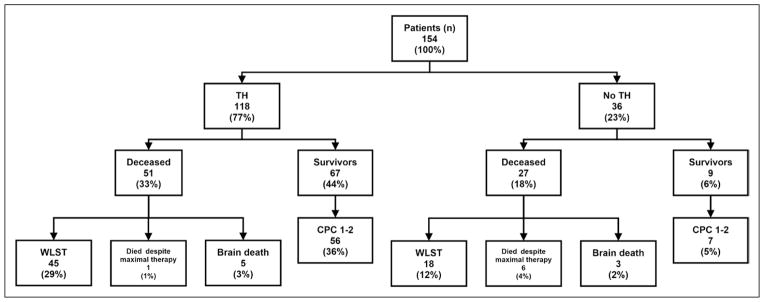
Measurements and main results: The study cohort included 154 comatose survivors of witnessed out-of-hospital cardiopulmonary arrests who were admitted to an ICU during the 54-month study period. One hundred eighteen patients (77%) were treated with therapeutic hypothermia. The mean age was 59 years, 104 (68%) were men, and 83 (54%) had an initial rhythm of ventricular tachycardia or fibrillation. Only eight of all 78 patients (10%) who died qualified as brain dead; and 81% of all patients (63 of 78) who died did so after withdrawal of life-sustaining treatment. Twenty of 56 comatose survivors (32%) treated with hypothermia who awoke (as defined by Glasgow Motor Score of 6) and had good neurologic outcomes (defined as Cerebral Performance Category 1-2) did so after 72 hours.
Conclusions: Our study supports delaying prognostication and withdrawal of life-sustaining treatment to beyond 72 hours in cases treated with therapeutic hypothermia. Larger multicenter prospective studies are needed to better define the most appropriate time frame for prognostication in comatose cardiac arrest survivors treated with therapeutic hypothermia. These data are also consistent with the notion that a majority of out-of-hospital cardiopulmonary arrest survivors die after a decision to withdrawal of life-sustaining treatment and that very few of these survivors progress to brain death.
Conflict of interest statement
The remaining authors have disclosed that they do not have any potential conflicts of interest.
Figures

Comment in
-
Prognosis after cardiac arrest: time to rethink why, how, and when*.Crit Care Med. 2014 Dec;42(12):2630-1. doi: 10.1097/CCM.0000000000000584. Crit Care Med. 2014. PMID: 25402283 No abstract available.
-
Neurologic assessment of comatose survivors of cardiac arrest: the details matter.Crit Care Med. 2015 Apr;43(4):e120-1. doi: 10.1097/CCM.0000000000000873. Crit Care Med. 2015. PMID: 25768370 No abstract available.
-
The authors reply.Crit Care Med. 2015 Apr;43(4):e121-2. doi: 10.1097/CCM.0000000000000898. Crit Care Med. 2015. PMID: 25768371 No abstract available.
References
-
- Neumar RW, Nolan JP, Adrie C, et al. Post-cardiac arrest syndrome: Epidemiology, pathophysiology, treatment, and prognostication. A consensus statement from the International Liaison Committee on Resuscitation (American Heart Association, Australian and New Zealand Council on Resuscitation, European Resuscitation Council, Heart and Stroke Foundation of Canada, InterAmerican Heart Foundation, Resuscitation Council of Asia, and the Resuscitation Council of Southern Africa); the American Heart Association Emergency Cardiovascular Care Committee; the Council on Cardiovascular Surgery and Anesthesia; the Council on Cardiopulmonary, Perioperative, and Critical Care; the Council on Clinical Cardiology; and the Stroke Council. Circulation. 2008;118:2452–2483. - PubMed
-
- Morrison LJ, Deakin CD, Morley PT, et al. Advanced Life Support Chapter Collaborators: Part 8: Advanced life support: 2010 International Consensus on Cardiopulmonary Resuscitation and Emergency Cardiovascular Care Science With Treatment Recommendations. Circulation. 2010;122:S345–S421. - PubMed
-
- Nolan JP, Soar J. Postresuscitation care: Entering a new era. Curr Opin Crit Care. 2010;16:216–222. - PubMed
-
- Hypothermia After Cardiac Arrest Group. Mild therapeutic hypothermia to improve the neurologic outcome after cardiac arrest. N Engl J Med. 2002;346:549–556. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
