

The frequency and determinants of liver stiffness measurement failure: a retrospective study of "real-life" 38,464 examinations
- PMID: 25122123
- PMCID: PMC4133303
- DOI: 10.1371/journal.pone.0105183
The frequency and determinants of liver stiffness measurement failure: a retrospective study of "real-life" 38,464 examinations
Abstract
Objective: To investigate the frequency and determinants of liver stiffness measurement (LSM) failure by means of FibroScan in "real-life" Chinese patients.
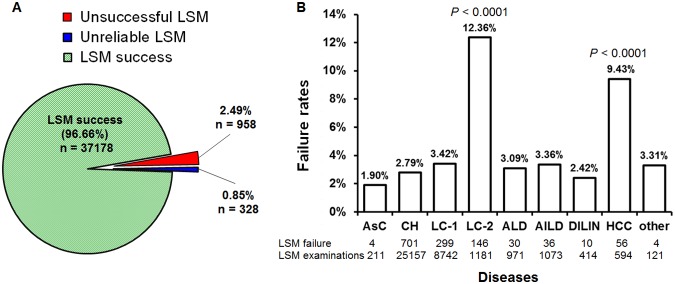
Methods: A total of 38,464 "real-life" Chinese patients in 302 military hospital of China through the whole year of 2013, including asymptomatic carrier, chronic hepatitis B, chronic hepatitis C, liver cirrhosis (LC), alcoholic liver disease, autoimmune liver disease, hepatocellular carcinoma (HCC) and other, were enrolled, their clinical and biological parameters were retrospectively investigated. Liver fibrosis was evaluated by FibroScan detection. S probe (for children with height less than 1.20 m) and M probe (for adults) were used. LSM failure defined as zero valid shots (unsuccessful LSM), or the ratio of the interquartile range to the median of 10 measurements (IQR/M) greater than 0.30 plus median LSM greater or equal to 7.1 kPa (unreliable LSM).
Results: LSM failure occurred in 3.34% of all examinations (1286 patients out of 38,464), among them, there were 958 cases (2.49%) with unsuccessful LSM, and 328 patients (0.85%) with unreliable LSM. Statistical analyses showed that LSM failure was independently associated with body mass index (BMI) greater than 30 kg/m(2), female sex, age greater than 50 years, intercostal spaces (IS) less than 9 mm, decompensated liver cirrhosis and HCC patients. There were no significant differences among other diseases. By changing another skilled operator, success was achieved on 301 cases out of 1286, which reduced the failure rate to 2.56%, the decrease was significant (P<0.0001).
Conclusions: The principal reasons of LSM failure are ascites, obesity and narrow of IS. The failure rates of HCC, decompensated LC, elder or female patients are higher. These results emphasize the need for adequate operator training, technological improvements and optimal criteria for specific patient subpopulations.
Conflict of interest statement
Figures


References
-
- Povero D, Busletta C, Novo E, di Bonzo LV, Cannito S, et al. (2010) Liver fibrosis: a dynamic and potentially reversible process. Histol Histopathol 25: 1075–1091. - PubMed
-
- Castera L (2012) Noninvasive methods to assess liver disease in patients with hepatitis B or C. Gastroenterology. 142: 1293–1302. - PubMed
-
- Duarte-Rojo A, Altamirano JT, Feld JJ (2012) Noninvasive markers of fibrosis: key concepts for improving accuracy in daily clinical practice. Ann Hepatol 11: 426–439. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
