

Cardiac structure and function and prognosis in heart failure with preserved ejection fraction: findings from the echocardiographic study of the Treatment of Preserved Cardiac Function Heart Failure with an Aldosterone Antagonist (TOPCAT) Trial
- PMID: 25122186
- PMCID: PMC4916914
- DOI: 10.1161/CIRCHEARTFAILURE.114.001583
Cardiac structure and function and prognosis in heart failure with preserved ejection fraction: findings from the echocardiographic study of the Treatment of Preserved Cardiac Function Heart Failure with an Aldosterone Antagonist (TOPCAT) Trial
Abstract
Background: Abnormalities in cardiac structure and function in heart failure with preserved ejection fraction may help identify patients at particularly high risk for cardiovascular morbidity and mortality.
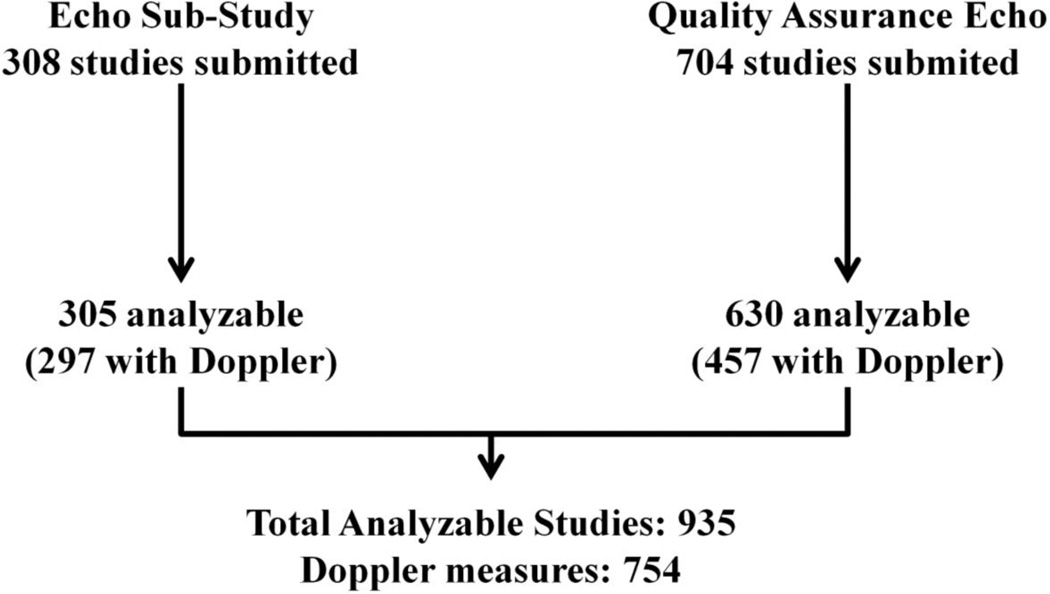
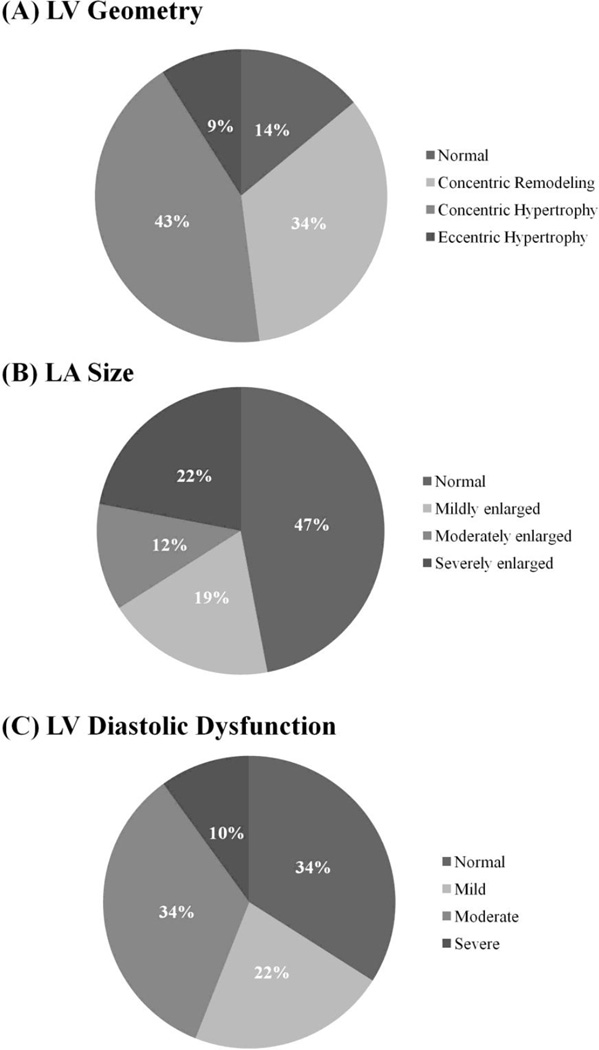
Methods and results: Cardiac structure and function were assessed by echocardiography in a blinded core laboratory at baseline in 935 patients with heart failure with preserved ejection fraction (left ventricular ejection fraction ≥45%) enrolled in the Treatment of Preserved Cardiac Function Heart Failure with an Aldosterone Antagonist (TOPCAT) trial and related to the primary composite outcome of cardiovascular death, heart failure hospitalization, or aborted cardiac arrest, and its components. At a median follow-up of 2.9 years, 244 patients experienced the primary outcome. Left ventricular hypertrophy (adjusted hazard ratio, 1.52; 95% confidence interval, 1.16-2.00), elevated left ventricular filling pressure (E/E'; adjusted hazard ratio 1.05 per 1 integer increase; 95% confidence interval, 1.02-1.07), and higher pulmonary artery pressure assessed by the tricuspid regurgitation velocity (hazard ratio, 1.23 per 0.5 m/s increase; 95% confidence interval, 1.02-1.49) were associated with the composite outcome and heart failure hospitalization alone after adjusting for clinical and laboratory variables. The risk of adverse outcome associated with left ventricular hypertrophy was additive to the risk associated with elevated E/E'.
Conclusions: Among heart failure with preserved ejection fraction patients enrolled in TOPCAT, left ventricular hypertrophy, higher left ventricular filling pressure, and higher pulmonary artery pressure were predictive of heart failure hospitalization, cardiovascular death, or aborted cardiac arrest independent of clinical and laboratory predictors. These features, both alone and in combination, identify heart failure with preserved ejection fraction patients at particularly high risk for cardiovascular morbidity and mortality.
Clinical trial registration url: http://www.clinicaltrials.gov. Unique identifier: NCT00094302.
Keywords: clinical trial; echocardiography; heart failure.
© 2014 American Heart Association, Inc.
Figures
References
-
- Bhatia RS, Tu JV, Lee DS, Austin PC, Fang J, Haouzi A, Gong Y, Liu P. Outcome of heart failure with preserved ejection fraction in a population-based study. New Engl J Med. 2006;355:260–269. - PubMed
-
- Owan TE, Hodge DO, Herges RM, Jacobsen SJ, Roger VL, Redfield MM. Trends in prevalence and outcome of heart failure with preserved ejection fraction. New Engl J Med. 2006;355:251–259. - PubMed
-
- Yusuf S, Pfeffer MA, Swedberg K, Granger CB, Held P, McMurray JJV, Michelson EL, Olofsson B, Ostergren J for the CHARM investigators and committees. Effects of candesartan in patients with chronic heart failure and preserved left-ventricular ejection fraction: the CHARM-Preserved Trial. Lancet. 2003;362:777–781. - PubMed
-
- Cleland JGF, Tendera M, Adamus J, Freemantle N, Polonski L, Taylor J on behalf of PEP-CHF investigators. The perindopril in elderly people with chronic heart failure (PEP-CHF) study. Eur Heart J. 2006;27:2338–2345. - PubMed
-
- Massie BM, Carson PE, McMurray JJ, Komajda M, McKelvie R, Zile MR, Anderson S, Donovan M, Iverson E, Staiger C, Ptaszynska A for the I-PRESERVE investigators. New Engl J Med. 2008;359:2456–2467. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
