

Targets for parathyroid hormone in secondary hyperparathyroidism: is a "one-size-fits-all" approach appropriate? A prospective incident cohort study
- PMID: 25123022
- PMCID: PMC4236624
- DOI: 10.1186/1471-2369-15-132
Targets for parathyroid hormone in secondary hyperparathyroidism: is a "one-size-fits-all" approach appropriate? A prospective incident cohort study
Abstract
Background: Recommendations for secondary hyperparathyroidism (SHPT) consider that a "one-size-fits-all" target enables efficacy of care. In routine clinical practice, SHPT continues to pose diagnosis and treatment challenges. One hypothesis that could explain these difficulties is that dialysis population with SHPT is not homogeneous.
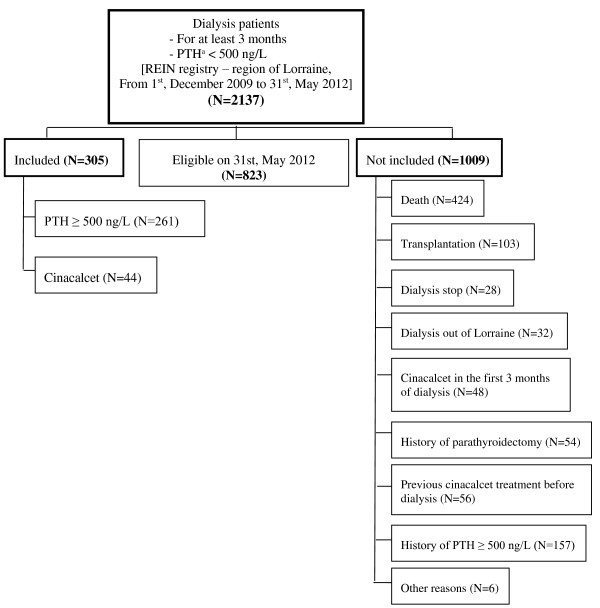
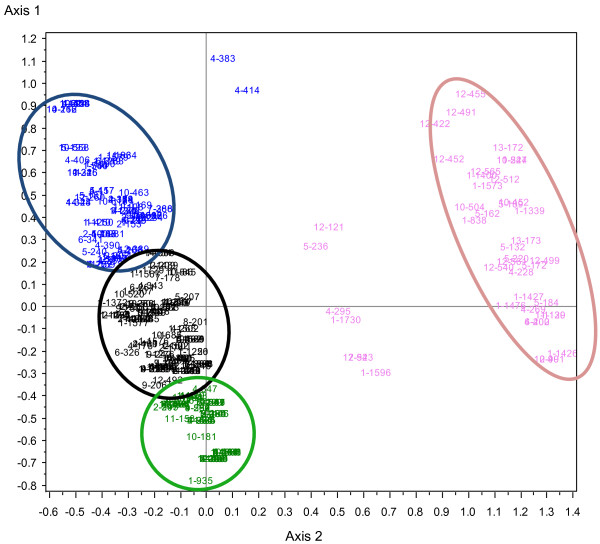
Methods: EPHEYL is a prospective, multicenter, pharmacoepidemiological study including chronic dialysis patients (≥ 3 months) with newly SHPT diagnosis, i.e. parathyroid hormone (PTH) ≥ 500 ng/L for the first time, or initiation of cinacalcet, or parathyroidectomy. Multiple correspondence analysis and ascendant hierarchical clustering on clinico-biological (symptoms, PTH, plasma phosphorus and alkaline phosphatase) and treatment of SHPT (cinacalcet, vitamin D, calcium, or calcium-free calcic phosphate binder) were performed to identify distinct phenotypes.
Results: 305 patients (261 with incident PTH ≥ 500 ng/L; 44 with cinacalcet initiation) were included. Their mean age was 67 ± 15 years, and 60% were men, 92% on hemodialysis and 8% on peritoneal dialysis. Four subgroups of SHPT patients were identified: 1/ "intermediate" phenotype with hyperphosphatemia without hypocalcemia (n = 113); 2/ younger patients with severe comorbidities, hyperphosphatemia and hypocalcemia, despite SHPT multiple medical treatments, suggesting poor adherence (n = 73); 3/ elderly patients with few cardiovascular comorbidities, controlled phospho-calcium balance, higher PTH, and few treatments (n = 75); 4/ patients who initiated cinacalcet (n = 43). The quality criterion of the model had a cut-off of 14 (>2), suggesting a relevant classification.
Conclusion: In real life, dialysis patients with newly diagnosed SHPT constitute a very heterogeneous population. A "one-size-fits-all" target approach is probably not appropriate. Therapeutic management needs to be adjusted to the 4 different phenotypes.
Figures
References
-
- Katz AI, Hampers CL, Merrill JP. Secondary hyperparathyroidism and renal osteodystrophy in chronic renal failure. Analysis of 195 patients, with observations on the effects of chronic dialysis, kidney transplantation and subtotal parathyroidectomy. Medicine (Baltimore) 1969;48:333–374. - PubMed
-
- Moe S, Druëke T, Cunningham J, Goodman W, Martin K, Olgaard K, Ott S, Sprague S, Lameire N, Eknoyan G. Definition, evaluation, and classification of renal osteodystrophy: A position statement from Kidney Disease: Improving Global Outcomes (KDIGO) Kidney Int. 2006;69:1945–1953. doi: 10.1038/sj.ki.5000414. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Other Literature Sources