

Haemodialysing babies weighing <8 kg with the Newcastle infant dialysis and ultrafiltration system (Nidus): comparison with peritoneal and conventional haemodialysis
- PMID: 25125229
- PMCID: PMC4167433
- DOI: 10.1007/s00467-014-2923-3
Haemodialysing babies weighing <8 kg with the Newcastle infant dialysis and ultrafiltration system (Nidus): comparison with peritoneal and conventional haemodialysis
Abstract
Background: To compare the efficacy of the Newcastle infant dialysis and ultrafiltration system (Nidus) with peritoneal dialysis (PD) and conventional haemodialysis (HD) in infants weighing <8 kg.
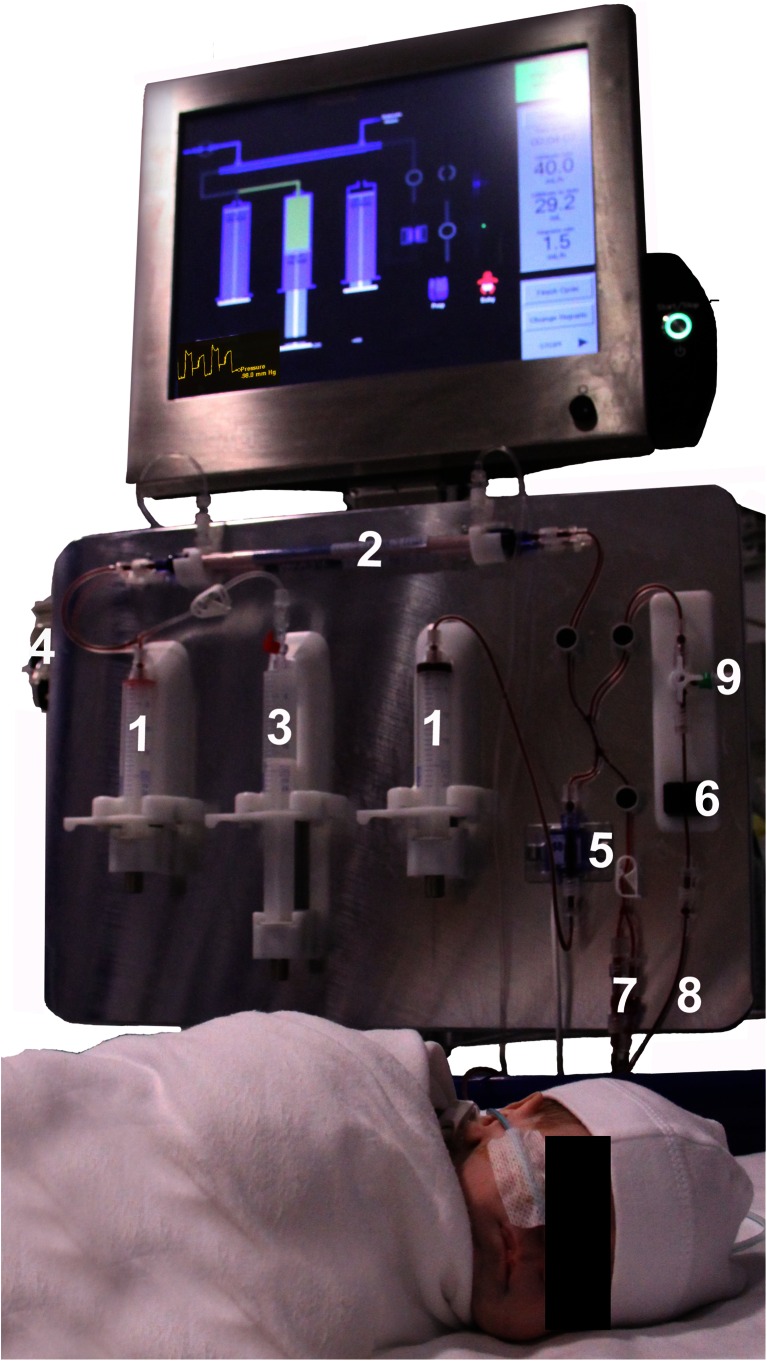
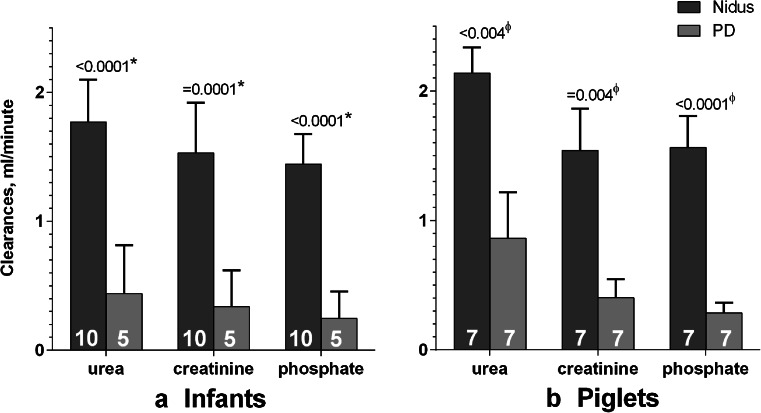
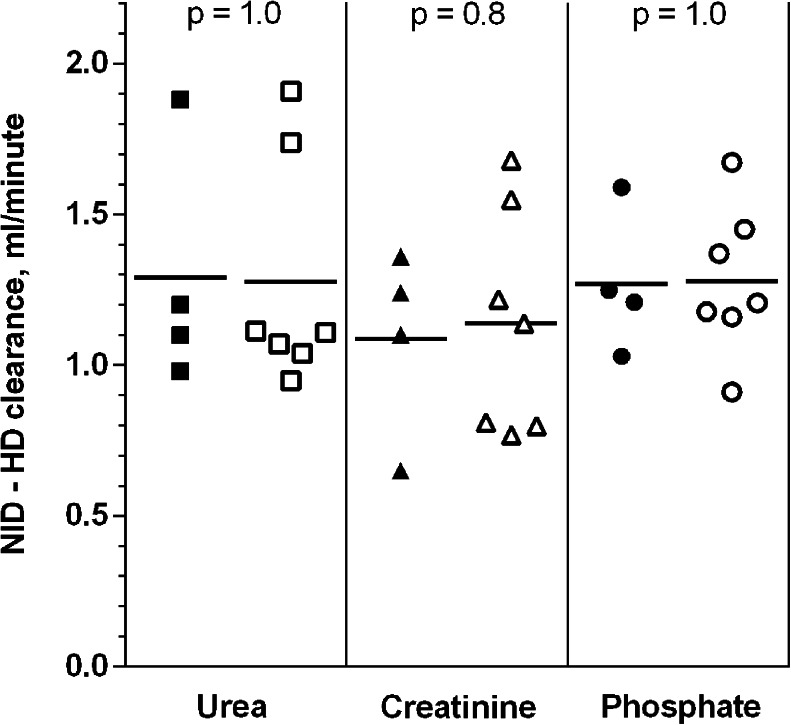
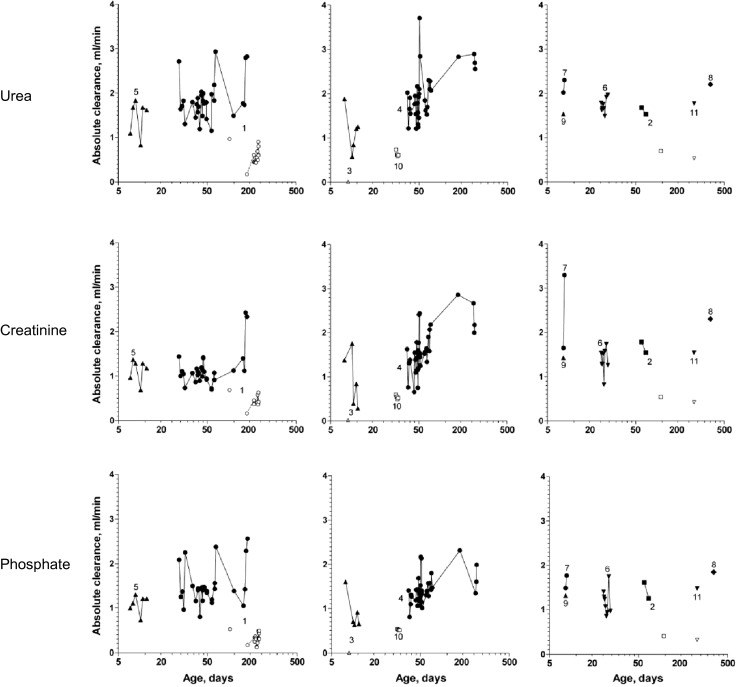
Methods: We compared the urea, creatinine and phosphate clearances, the ultrafiltration precision, and the safety of the Nidus machine with PD in 7 piglets weighing 1-8 kg, in a planned randomised cross-over trial in babies, and in babies for whom no other therapy existed, some of whom later graduated to conventional HD.
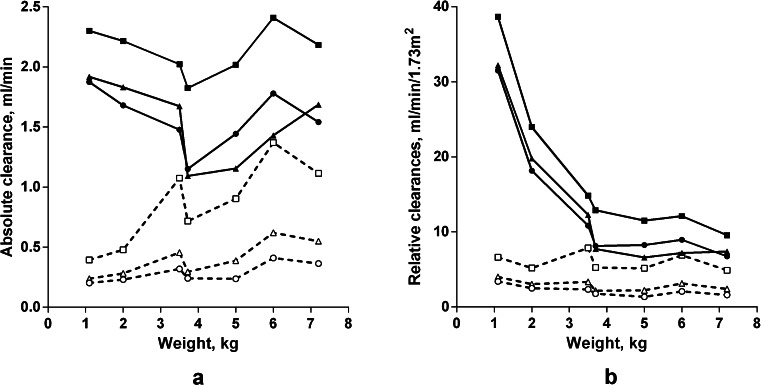
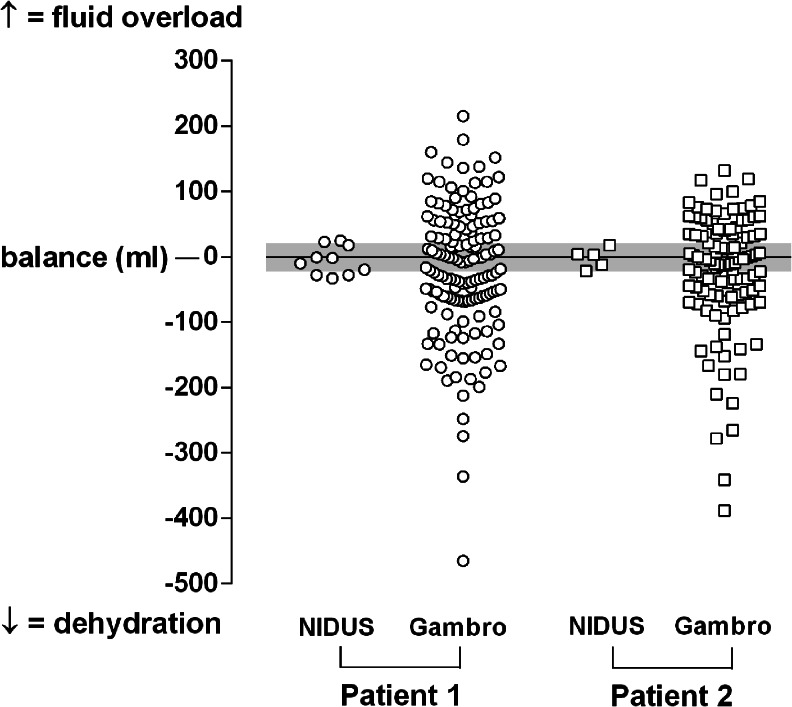
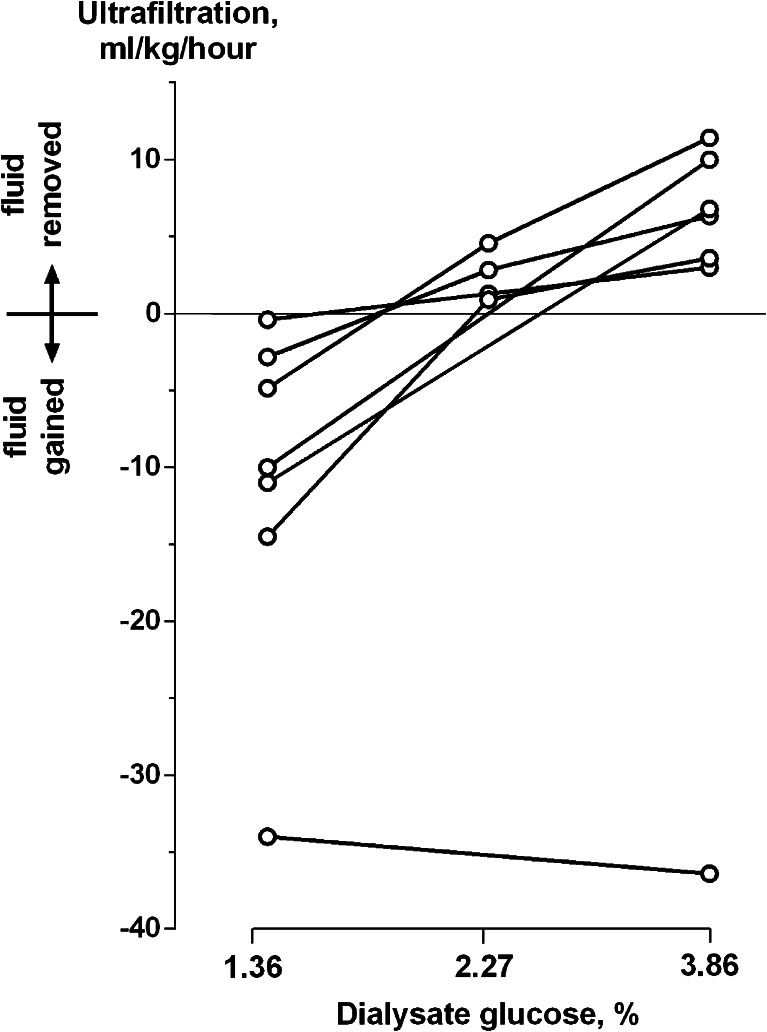
Results: Two babies entered the randomised trial; 1 recovered rapidly on PD, the other remained on the Nidus as PD failed. Additionally, 9 babies were treated on the Nidus on humanitarian grounds: 3 because of failed PD, and 3 with permanent kidney failure later converted to conventional HD. We haemodialysed 10 babies weighing between 1.8 and 5.9 kg for 2,475 h during 354 Nidus sessions without any clinically important incidents, and without detectable haemolysis. Single-lumen vascular access was used with no blood priming of circuits. The urea, creatinine and phosphate clearances using the Nidus were around 1.5 to 2.0 ml/min in piglets and babies, and were consistently higher than PD clearances, which ranged from about 0.2 to 0.8 ml/min (p ≤ 0.0002 for each chemical). Ultrafiltration was achieved to microlitre precision by the Nidus, but varied widely with PD. Fluid removal using conventional HD was imprecise and resulted in some hypovolaemic episodes requiring correction.
Conclusion: The Nidus can provide HD in the Pediatric Intensive Care Unit (PICU) and outpatient intermittent HD without blood priming for babies weighing <8 kg, It generates higher dialysis clearances than PD, and delivers more precise ultrafiltration control than either PD or conventional HD.
Figures
Comment in
-
Designing technology to meet the therapeutic demands of acute renal injury in neonates and small infants.Pediatr Nephrol. 2014 Oct;29(10):1869-71. doi: 10.1007/s00467-014-2910-8. Epub 2014 Aug 16. Pediatr Nephrol. 2014. PMID: 25125227
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
