

Hearing function in patients living with HIV/AIDS
- PMID: 25127320
- PMCID: PMC4208942
- DOI: 10.1097/AUD.0000000000000064
Hearing function in patients living with HIV/AIDS
Abstract
Objectives: During the earlier years of the HIV/AIDS epidemic, initial reports described sensorineural hearing loss in up to 49% of individuals with HIV/AIDS. During those years, patients commonly progressed to advanced stages of HIV disease and frequently had neurological complications. However, the abnormalities on pure-tone audiometry and brainstem-evoked responses outlined in small studies were not always consistently correlated with advanced stages of HIV/AIDS. Moreover, these studies could not exclude the confounding effect of concurrent opportunistic infections and syphilis. Additional reports also have indicated that some antiretroviral medications may be ototoxic; thus, it has been difficult to make conclusions regarding the cause of changes in hearing function in HIV-infected patients. More recently, accelerated aging has been suggested as a potential explanation for the disproportionate increase in complications of aging described in many HIV-infected patients; hence, accelerated aging-associated hearing loss may also be playing a role in these patients.
Design: We conducted a large cross-sectional analysis of hearing function in over 300 patients with HIV-1 infection and in 137 HIV-uninfected controls. HIV-infected participants and HIV-uninfected controls underwent a 2-hr battery of hearing tests including the Hearing Handicap Inventory, standard audiometric pure-tone air and bone conduction testing, tympanometric testing, and speech reception and discrimination testing.
Results: Three-way analysis of variance (ANOVA) and logistic regression analysis of 278 eligible HIV-infected subjects stratified by disease stage in early HIV disease (n = 127) and late HIV disease (n = 148) and 120 eligible HIV-uninfected controls revealed no statistically significant differences among the three study groups in either overall 4-frequency pure-tone average (4-PTA) or hearing loss prevalence in either ear. Three-way ANOVA showed significant differences in word recognition scores in the right ear among groups, a significant group effect on tympanogram static admittance in both ears and a significant group effect on tympanic gradient in the right ear. There was significantly larger admittance and gradient in controls as compared to the HIV-infected group at late stage of disease. Hearing loss in the HIV-infected groups was associated with increased age and was similar to that described in the literature for the general population. Three-way ANOVA analysis also indicated significantly greater pure-tone thresholds (worse hearing) at low frequencies in HIV patients in the late stage of disease compared with HIV-uninfected controls. This difference was also found by semi-parametric mixed effects models.
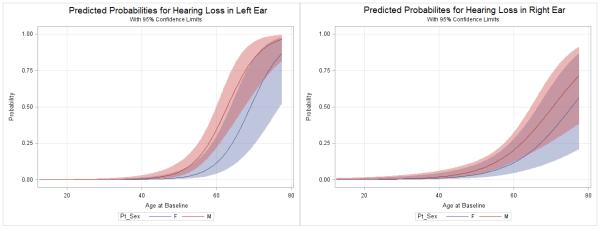
Conclusions: Despite reports of "premature" or "accelerated" aging in HIV-infected subjects, we found no evidence of hearing loss occurring at an earlier age in HIV-infected patients compared to HIV-uninfected controls. Similar to what is described in the general population, the probability of hearing loss increased with age in the HIV-infected subjects and was more common in patients over 60 years of age. Interestingly, HIV-infected subjects had worse hearing at lower frequencies and have significant differences in tympanometry compared to HIV-uninfected controls; these findings deserve further study.
Figures
References
-
- Bai U, Seidman MD, Hinojosa R, et al. Mitochondrial DNA deletions associated with aging and possibly presbycusis: a human archival temporal bone study. Am J Otol. 1997 Jul;18(4):449–453. - PubMed
-
- Bergmeyer, Gregory Au.D., OSHA [Accessed September 2009];Recordable Questionnaire from the Adventist Medical Center at Portland, OR. http://www.adventisthealthnw.com/services-and-programs/audiology-forms.
-
- Dai P, Yang W, Jiang S, et al. Correlation of cochlear blood supply with mitochondrial DNA common deletion in presbyacusis. Acta Otolaryngol. 2004 Mar;124(2):130–6. - PubMed
-
- Deeks SG, Verdin E, McCune JM. Immunosenescence and HIV. Curr Opin Immunol. 2012 Aug;24(4):501–6. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
